
The rationale for derisking DMTs
How can I derisk or reduce my chances of getting certain adverse events on specific DMTs, in particular alemtuzumab or AHSCT?

Case study
I am a 34-year-old woman with highly active MS. I have been on dimethyl fumarate for over a year and have had two severe relapses. Three months ago, I developed numbness in my feet that ascended to just below my rib cage. Shortly after, I became weak in my legs and lost bladder function. I was admitted to my local hospital and was treated with two courses of high-dose intravenous steroids. I gradually made a recovery and was discharged with a home rehabilitation programme. Then, three weeks ago, over 12 hours I developed severe nausea, vomiting, double vision, vertigo and unsteadiness of gait. I saw my neurologist, who has now diagnosed me with brainstem relapse. My MRI has revealed over ten new brain lesions with several enhancing lesions and a new lesion in my thoracic spine. My consultant has recommended I be treated with alemtuzumab and/or AHSCT. However, after reading about the risks of these treatments, I am not sure I am prepared to take them. What would you advise?

Prof G’s opinion
Based on the limited information you have provided me, I can see why your neurologist has recommended the most effective disease-modifying therapies (alemtuzumab) and AHSCT. You have failed a platform therapy and have had two disabling attacks within a 12-month period with MRI evidence of active disease. Based on this, we would classify you as having rapidly evolving severe (RES) MS. Under our current NHS England Guideline, you would be eligible to switch to any of the higher efficacy DMTs (natalizumab, fingolimod, ocrelizumab, ofatumumab, cladribine, alemtuzumab). However, under the current Pan-London AHSCT guidelines, you would not be eligible for AHSCT as DMF is not classified as a high-efficacy DMT. If you live outside of the UK, access to AHCT may not be restricted by this criterion. If you are living in the UK, you may be eligible for the STAR-MS trial that is comparing AHSCT to other high-efficacy DMTs.
Before rushing into a switch, I suggest you pause and go back to basics. I recommend you start by going through all my previous newsletters, so you know the answers to the questions below.
What is the risk of not being treated with a disease-modifying therapy (DMT)?
What are the attributes of the specific DMTs or treatment strategies?
Natalizumab
S1P modulators
Alemtuzumab
Teriflunomide
Fumarates
Anti-CD20
AHSCT
How can I derisk or reduce my chances of getting certain adverse events on specific DMTs?
Will I be able to become a parent? What about pregnancy and breastfeeding?
I have done a separate Newsletter comparing alemtuzumab to AHSCT (20-7-2021), which you may also find helpful.
Summary
I do think you need to be treated ASAP. You are at risk of having a further catastrophic relapse while waiting to be treated, for example, with AHSCT. The downside of AHSCT is that it is not a treatment that can be started next week. In reality, it takes six months or more to have AHSCT on the NHS. Why? You first need to have your case reviewed by the Pan-London AHSCT MDT (multi-disciplinary team); this takes anything from 2 to 8 weeks. Once they agree you are eligible, you need to be seen in our local MS-AHSCT clinic by a neurologist and a haematologist. If you are planning to start or extend a family, you need to be referred to a local fertility clinic for harvesting and storing your eggs (or sperm if you are a male). In my experience, egg harvesting and storage takes 2-3 months on the NHS. In addition to this, you need to have baseline blood tests done. You then need to be given a date for the first phase of AHSCT, i.e. the mobilisation and harvesting of the stem cells. This is followed two to three weeks later by admission to the bone marrow transplant unit for the ablation and stem cell transplant. Depending on how quickly your bone marrow function recovers and whether or not you have any complications from the procedure, you may spend 3-4 weeks in the hospital and occasionally longer if there are complications.
In comparison, alemtuzumab can usually be started within 4-6 weeks. In our centre, your case needs to be presented at our MS MDT for approval, we need to get all your baseline blood tests done and if necessary get you vaccinated against some of the viruses that may cause problems when you are immunodepleted, for example, varicella-zoster virus (VZV). A major advantage of alemtuzumab, and other IRTs, is that any non-urgent vaccines can be given later when you have reconstituted your immune system. With continuous immunosuppressive therapies, this is not possible.
If you need time to think about things, I would consider asking your neurologist to start you on natalizumab and to have at least six months of treatment whilst you decide on your long-term treatment strategy. Natalizumab is our fastest acting highly efficacy DMT. It has a reversible mode of action, i.e. it does not alter the immune system irrevocably, so it is an ideal DMT to use in this way.
How to derisk or reduce your chances of getting certain adverse events on specific DMTs?
Disease-modifying therapies (DMTs) can be classified as being immunosuppressive or not. The latter are immunomodulatory DMTs and include interferon-beta, glatiramer acetate and arguably teriflunomide. Broadly speaking, an immunosuppressive is any DMT that reduces the activation or effectiveness, of the immune system.
From a regulatory perspective, for a drug to be classified as being immunosuppressive, it should:
Cause significant lymphopaenia or leukopenia (reduced white cell counts).
Be associated with opportunistic infections, infections that don’t occur in people with a normal immune system.
Reduce antibody and/or T-cell responses to vaccines.
Increase the risk of secondary malignancies.
The duration and intensity of immunosuppression further determine the risks. For example, short-term or intermittent immunosuppression associated with an immune reconstitution therapy (IRT) front-load the risks, which are substantially lower once the immune system has reconstituted itself. In comparison, long-term continuous or persistent immunosuppression, which occurs with most of the maintenance DMTs, accumulates problems over time, particularly opportunistic infections and secondary malignancies.
Immunosuppression that accompanies the DMTs can be selective or non-selective. Non-selective refers to therapies that deplete and/or suppress the adaptive (T and B cells) and the innate immune system (monocytes, neutrophils and natural killer cells or NK cells). Alemtuzumab, HSCT and mitoxantrone are non-selective and are therefore associated with acute bacterial infections such as Listeriosis, Nocardiosis and cytomegalovirus (CMV) reactivation. In comparison, anti-CD20 (ocrelizumab, ofatumumab) and cladribine are selective, i.e. they don't affect the innate immune system, and are therefore associated with a low risk of acute bacterial infections.
The table summarises the main characteristics of intermittent and persistent immunosuppression. Live vaccines are, in general, contraindicated in patients on continuous immunosuppressive therapies. In comparison, pwMS on IRTs who have reconstituted their immune systems can tolerate and respond to live vaccines. The decision to administer live vaccines always needs to be balanced against the risks of the vaccine.

Please note that the consequences of immunosuppression are not black-and-white and interact with other factors such as ageing (immunosenescence), carryover effects from previous DMTs, concomitant medications, comorbidities (smoking, obesity, diabetes, sedentary lifestyle, etc.), disability and social determinants of health such as levels of deprivation and the lived environment. These factors have been particularly highlighted in the COVID-19 pandemic regarding the risk of getting severe COVID-19 and COVID-19 vaccine responses, including the rate of the waning of the immune response.
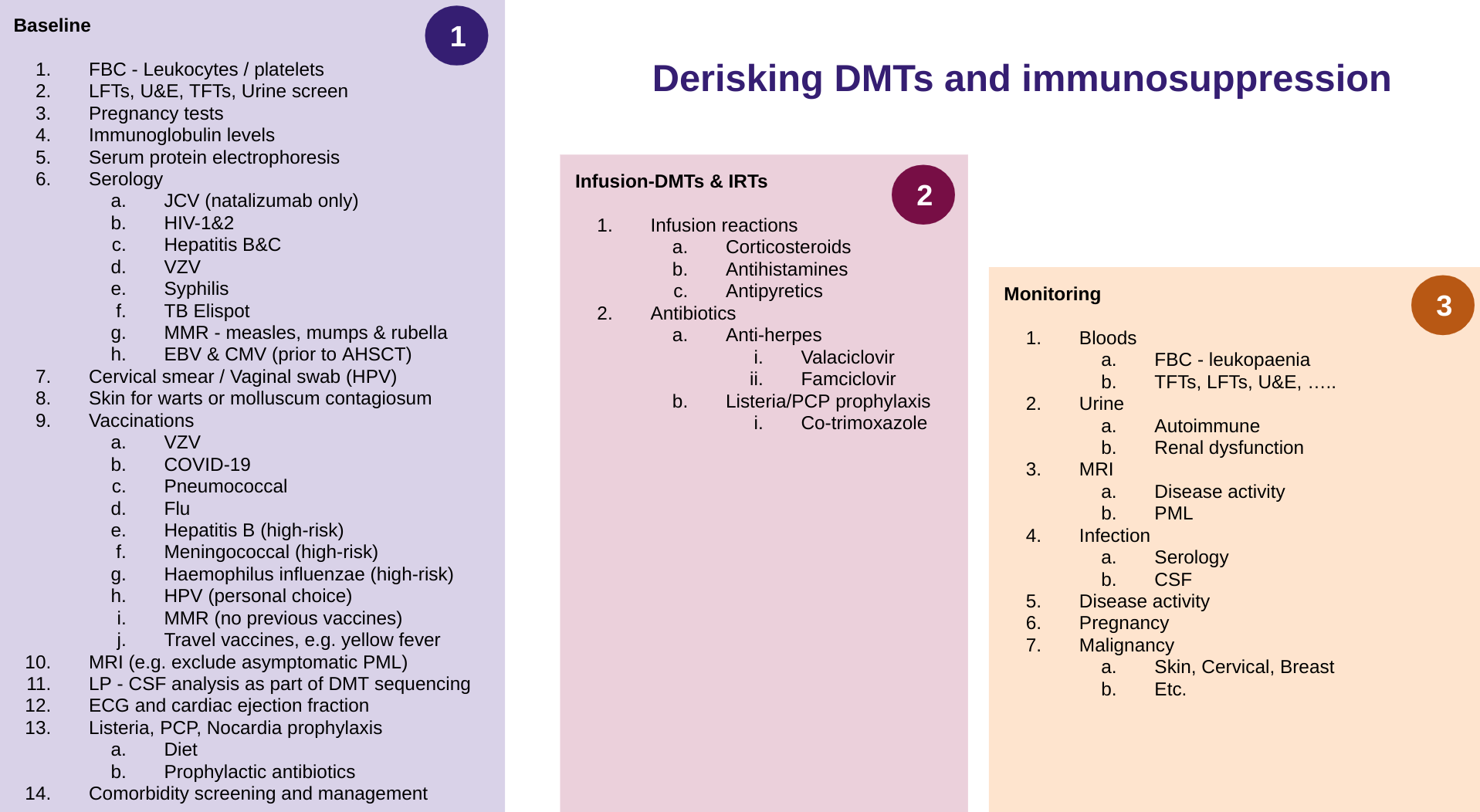
You need to realise that we can de-risk many of the complications associated with long-term immunosuppression and the use of DMTs. The following list summarises what needs to be done at baseline during the administration of DMTs and monitoring. The specifics, however, vary from DMT to DMT. We generally do baseline blood and urine tests to ensure they are normal. These include your full blood count, platelets, liver, renal and thyroid function tests, and a urine screen. We also check baseline immunoglobulin levels; this is particularly important if you are about to start an anti-CD20 therapy (ocrelizumab or ofatumumab) so we have a reference level for future comparisons.
Serum protein electrophoresis is done for patients considering starting interferon-beta; having a so-called monoclonal gammopathy (an abnormal immunoglobulin) is a contraindication to starting an interferon-beta formulation. There have been several deaths of pwMS with monoclonal gammopathies dying from a rare lung complication when starting interferon beta. This complication is due to a form of capillary leak syndrome, and these people get acute adult respiratory distress syndrome, which is usually life-threatening.
At our centre, we do a relatively large infectious screen to ensure you don’t have a subclinical infection that needs to be treated before starting your DMT, this is particularly relevant for HIV-1& 2, hepatitis B and C, syphilis and TB (tuberculosis). If we detect one of these infections, this delays us starting the DMT, as treatment needs to be started for these infections before you start the DMT.
JCV, the virus that causes PML (progressive multifocal leukoencephalopathy), is only really needed for pwMS considering starting natalizumab. Please note that even if you are JCV positive, you can still be treated with natalizumab for six to 12 months and sometimes beyond this if you are prepared to take on the risk and the extra monitoring required to detect PML early.
For patients starting long-term immunosuppression, it is a good idea to screen for active HPV infection (cervical smear or vaginal swab) and to make sure you don’t have warts or active infection with molluscum contagiosum. Warts are due to HPV skin infection and molluscum contagiosum due to a relatively benign pox virus infection that typically affects young children. However, adults can rarely be affected by molluscum contagiosum. I have seen warts and molluscum contagiosum spread rapidly in patients treated with alemtuzumab. In my opinion, these usually benign viral skin infections should be treated before patients start immunosuppressive therapies, in particular, alemtuzumab.
Please note that we only check MMR status in patients with no documentation of being fully vaccinated as children (see ‘MMR vaccine: to vaccinate or not?’ 8-Aug-2022). We check VZV status before starting immunosuppression and vaccinate those who are seronegative. Currently, we are still using the live VZV vaccine. Shortly, this will change, and we will likely be offering all pwMS the component inactive VZV vaccine (Shingrex) that has recently had its licence extended to reduce the chances of zoster reactivation in all adults starting immunosuppression. This new Shringex indication is similar to the pneumococcal vaccine (Pneumovax). We are only recommending Pneumovax in patients about to start an anti-CD20. However, when Shringex becomes available on the NHS, it will make sense to bundle this with the Pneumovax and make it routine for all pwMS before starting immunosuppressive therapy.
We encourage all patients to be vaccinated against COVID-19 and seasonal flu. The flu vaccine is only available between October and January each year, and if outside the flu vaccine season, we simply remind you to get vaccinated during the next vaccine season.
Hepatitis B, meningococcal and Haemophilus influenzae vaccines are only considered for pwMS who are at high-risk and have not had these vaccines as part of the national vaccine programme, i.e. healthcare and laboratory workers for hepatitis B, school and university students and military recruits for meningococcal vaccine and paediatric patients for Haemophilus influenzae.
The issue around having the HPV vaccine as an adult is more complex as the NHS does not cover the vaccine for people over 25. In addition, most people have only had the quadrivalent vaccine (Gardasil-4), which only covers about two-thirds of the strains that cause cancer. They now want to upgrade their immunity with the polyvalent vaccine (Gardasil-9) that covers over 95% of the cancer-causing strains of HPV. We are seeing an increasing number of pwMS opting for or upgrading their immunity with the newer polyvalent vaccine (Gardasil-9). For more information on HPV vaccination, please see ‘Case study: cervical intraepithelial neoplasia (CIN) and ocrelizumab’, 6-Nov-2021.
Another issue is travel vaccines for people who have to travel as part of their work or are planning to travel shortly. The one vaccine that needs to be discussed is the yellow fever vaccine which is a live vaccine and should ideally be given before someone starts on immunosuppressive therapy.
Please note routine EBV and CMV status and monitoring are only needed for subjects undergoing AHSCT, which causes a more profound short-term immunosuppression that can result in both CMV and EBV reactivation. CMV reactivation also happens with alemtuzumab and needs to be considered when investigating patients who develop complications after alemtuzumab (Please see ‘Opportunistic infection in MS’ 15-Jul-2022).
Prophylactic antivirals and antibiotics
For patients undergoing AHSCT or receiving alemtuzumab, we cover them with antivirals and antibiotics to reduce the chances of getting certain infections. This is particularly relevant for Listeriosis, which is an uncommon infection that is transmitted via food. We also encourage all our patients to start and maintain a specific diet to reduce the chances of getting Listeriosis. Please note that the risk of Listeriosis is only present for a short period when both the adaptive and innate immune systems are compromised, i.e. four weeks after alemtuzumab. This is why we only recommend antibiotic prophylaxis for four weeks. I recommend you visit our online resource that covers Listeriosis, and if you live in the UK, you could order our Listeriosis prevention kit.
Cardiovascular screening
You will see from the list that you may have to have an ECG (electrocardiogram), and your left ventricular function checked (ejection fraction). The ECG is done to ensure you don’t have an abnormal heart rhythm or electrical conduction abnormality in the heart. These are a relative contraindication to using the S1P modulators (fingolimod, siponimod, ozanimod, ponesimod) that may affect the conduction of the heart. The left ventricular ejection fraction (LVEF) must be done at baseline and regularly in patients treated with mitoxantrone. Mitoxantrone is toxic to the heart, and we need to monitor for this. If there is a significant drop in the LVEF further dosing of mitoxantrone is contraindicated.
Pregnancy and family planning
Many chemotherapy agents used in AHSCT for ablating the bone marrow are toxic to the ovaries and testes. This is why patients have to be counselled before treatment and allowed to have eggs (oocytes) or sperm banked for future use. This egg banking is also an issue for pwMS being treated with mitoxantrone. As mitoxantrone does not cross the testes-blood barrier, men receiving mitoxantrone don’t require sperm banking.
Pharmacogenomics
This is only required at present for siponimod. Siponimod is metabolised by a specific liver enzyme with two functional variants, i.e. slow and fast metabolising variants. If you carry two slow metabolising variants of the enzyme, you cannot receive Siponimod. Intermediate metabolizers, i.e. those that carry one slow and one fast metabolising version of the enzyme, receive low-dose siponimod. In comparison, those with two fast metabolising enzymes receive high-dose siponimod.
Carryover PML
You will see that I have included MRI and a lumbar puncture with CSF JCV testing on the baseline tests. This is specific to patients at high risk of getting PML and are switching from natalizumab to a depleting IRT such as alemtuzumab or another immunosuppressive therapy. The reason for doing these tests is to exclude asymptomatic PML, which will be carried over onto the new treatment. This concerns patients who are to be treated with a therapy that depletes their immune system, such as alemtuzumab, cladribine or an anti-CD20 therapy. The effects of these therapies on your immune system can’t be rapidly reversed, which is a problem as immune reconstitution is needed to clear PML. It is debatable if CSF analysis is needed in this setting because you can still have PML and a negative CSF. This is why most MS centres don’t mandate CSF testing in this situation. I still request this test on my patients; when taking risks with one of your patient’s life, having as much information as possible is reassuring. Maybe I am wrong?
Infusion reactions
Many of you will be aware that when you use agents that cause cell lysis, i.e. alemtuzumab and intravenous anti-CD20 therapies, the contents of cells cause infusion reactions. To prevent infusion reactions or reduce their severity, we pretreat patients with corticosteroids, antihistamines and antipyretics. The exact protocols for each agent differ, and many centres have modified the protocols. For example, with ocrelizumab, the infusion reactions are only really a problem with the first and second infusions, and many centres don’t give steroids with the third and subsequent infusions. The latter was particularly important during the COVID-19 pandemic when it was shown that the recent administration of high-dose steroids increased your chances of getting severe COVID-19.
Ongoing monitoring
As you will see, once someone who has been treated with a DMT, ongoing monitoring is required. What gets monitored and how frequently it needs monitoring depends on the individual DMT. The regulatory authorities usually put in place specific monitoring requirements, which can differ worldwide. It is important that you also enrol in your national cancer screening programmes. Being on chronic immunosuppression increases your chances of getting secondary malignancies, so please remain vigilant.
I want to reassure you that all licensed MS DMTs have had a thorough risk-benefit assessment done by the drug regulators, and the benefits of these treatments are considered to outweigh the potential risks. On balance, the level of immunosuppression associated with MS DMTs is typically mild to moderate; hence, the complications are relatively uncommon. MS is a bad disease and, if left to run its natural course, would result in the vast majority of patients becoming disabled. I would not hesitate to guide this patient onto a high-efficacy DMT. Based on her history, both alemtuzumab and AHSCT seem appropriate. However, many other factors must be considered before making a definitive recommendation.
Subscriptions and donations
Paid subscriptions to MS-Selfie are being used to administer the Newsletter and associated MS-Selfie microsite currently in development. At the request of several readers, I have now added the option of making a one-off donation. To keep this initiative open to all readers, I would appreciate it if those who can afford a subscription please subscribe. For active paying subscribers, thank you; your contribution is much appreciated.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust. The advice is general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.
Astoundingly comprehensive, thank you!
Hello,
I realize that you are researching the correlation of EBV, and Multiple Sclerosis, the former contributing to the development of MS; other research centres are considering an EBV vaccine to ameliorate MS such as this one in Seattle:
https://www.facebook.com/sharer/sharer.php?u=https%3A%2F%2Fwww.fredhutch.org%2Fcontent%2Fwww%2Fen%2Fnews%2Fcenter-news%2F2022%2F06%2Fepstein-barr-vaccine-multiple-sclerosis.html
I really hope that we will gain access to EBV vaccines soon!