
How do I want my MS to be treated?
The newsletter addresses the differences between maintenance-escalation disease-modifying therapies and immune reconstitution therapies (IRTs) and why it is important to know about this distinction.

Many of my patients ask me if I had MS how would I want to be treated. This is a very difficult question and depends on your life stage, what risks you are prepared to take and having a deep understanding of what MS is and how we approach its treatment. In this Newsletter I try and address question 9 in my list of questions you need to ask yourself and understand before deciding on and starting a DMT.

How do I want my MS to be treated? What is the difference between a maintenance/escalation DMT and an IRT (immune reconstitution therapy)?
How can I reduce my chances of adverse events on specific DMTs?
What are the attributes of the specific DMTs or treatment strategies?
Will I be able to become a parent? What about pregnancy and breastfeeding?
Currently, there are two main treatment philosophies when it comes to treating MS with disease-modifying therapies (DMTs); maintenance-escalation vs. immune reconstitution therapies (IRTs).
What is an IRT?
By definition an IRT is given as a short course, i.e. as a one-off treatment in the case of AHSCT or intermittently as in the case of alemtuzumab, cladribine or mitoxantrone. IRTs are not given continuously and additional courses of the therapy are only given if there is a recurrence of MS inflammatory activity. IRTs have the ability to induce long-term remission and, arguably, in some cases a potential cure. Cynics would argue that none of our DMTs or treatments cure MS, but unless we define what constitutes a cure and look for it we won’t find it.
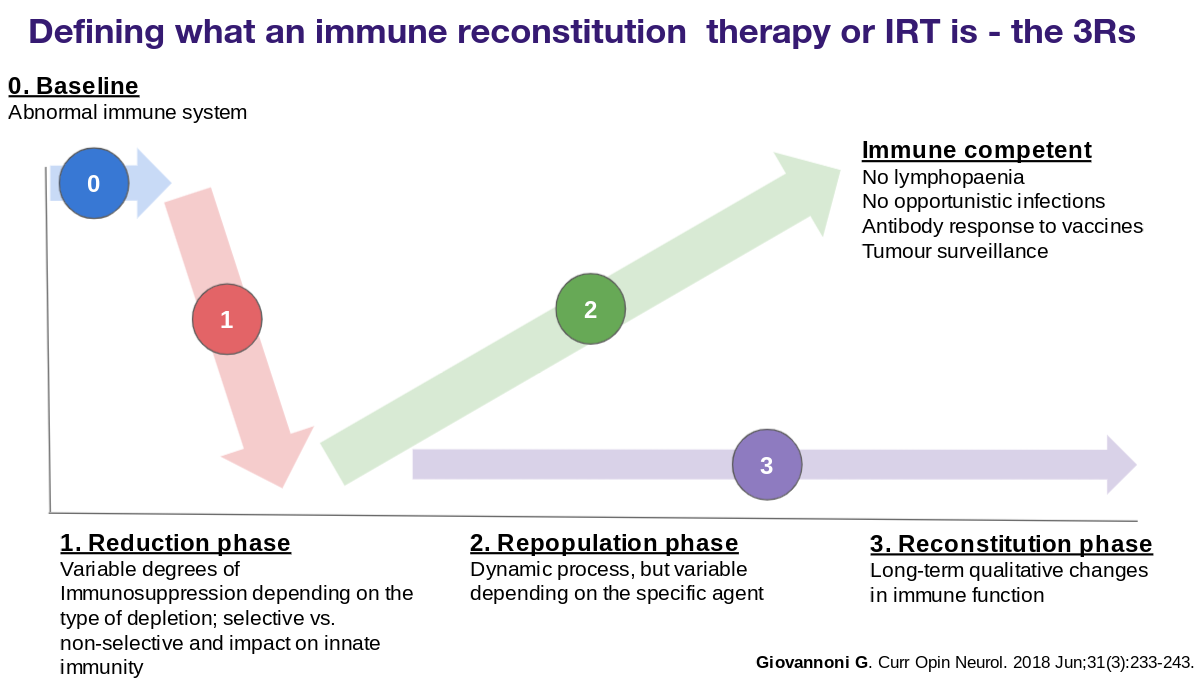
IRTs have three phases to their mode of action, which I refer to as the three Rs. The first phase is the reduction or the depletion phase in which we try and kill the autoimmune cells that cause MS. The second phase is the repopulation phase when the immune cell recovers from stem cells and hopefully, the autoimmune cells don’t return. The final phase is the reconstituted phase when the immune system is recovered and fully competent. Please note that the recovered immune system at the end of a treatment cycle with an IRT is different to what was there before the IRT. Some people like to think of an IRT as a reboot of the immune system, but without MS.
What is an MS "cure"?
One attempt defines an MS cure as no evident disease activity (NEDA) 15 years after the administration of an IRT. I justify using 15 years as it is the most commonly accepted time-point for defining 'benign MS' and happens to be beyond average time to the onset of secondary progressive MS in natural history studies.

What is maintenance therapy?
In comparison, a maintenance therapy by definition is given continuously without an interruption in dosing. Although maintenance therapies have the ability to induce long-term remission, i.e. NEDA, they cannot by definition result in a cure. With maintenance therapies, the recurrence of, or ongoing, inflammatory activity, is an indication that there is a suboptimal response to treatment and typically results in a treatment switch. Ideally, this switch should be to a more effective class of DMTs, hence the term escalation.
What would I recommend?
I can't choose for you. The debate between being treated with maintenance therapy and an IRT is complex and depends on many factors. The table below highlights key differentiators. One factor that is uppermost in most peoples’ minds at the moment is vaccine readiness, i.e. will I be able to mount an adequate immune response to a vaccine. IRTs have the advantage in that they allow reconstitution of the immune system and once it recovers vaccine responses are restored and even live vaccines can be given.
The best way to understand the complexities around the choice between these two options is to analysing some of the case studies that I have been discussed on this site. It is vital to understand the difference between continuous long term and short-term intermittent immunosuppression.

The future
In the future I envisage two more treatment strategies emerging. The first is induction-maintenance when we will use an IRT and follow it with a safer immunomodulatory therapy that is not immunosuppressive with the objective to keep MS in long-term remission. This approach is used in oncology, i.e. hit the cancer hard with induction chemotherapy and then keep the cancer at bay with a maintenance therapy that is safe and well-tolerated, for example, anti-hormonal therapies in breast cancer. The other approach is combination therapies; the aim would be to combine an anti-inflammatory therapy with say neuroprotective therapies to target smouldering MS.

I would be interested to know which treatment approach you think is most appealing.
Subscriptions
I am encouraging readers to subscribe to the MS-Selfie Newsletter. The subscriptions will give you access to the case studies and the full archive. Please note all other newsletters, such as this one, are free. The money from subscriptions will be used to employ somebody to administer, transfer and curate the contents of the Newsletter onto a companion MS-Selfie microsite. The objective is to create an MS self-help guide.
The MS-Selfie case study from the 7th of October is about a patient with rapidly evolving severe MS who was denied the option of an IRT by her neurologist because he thought it was too risky. This case study raises many issues about who is responsible for deciding what treatment strategy to adopt and who takes the risk; the HCP or the patient? You tell me!
Please note if you have MS and can’t afford the subscription please drop me an email and I can arrange a complimentary one.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust. The advice is intended as general advice and should not be interpreted as being personal clinical advice. If you have problems please tell your own healthcare professional who will be able to help you.
If I was at the start of my MS journey I would seriously consider an IRT. However, having had MS for over 25 years and successfully maintained by natalizumab at this stage of life I will stick with my current treatment. However I believe an IRT is a very serious contender for newly diagnosed. Hit it hard and hope it’s a ‘cure’.
My feeling on this is that most patients strive for a cure, to be fixed, or at least the closest thing. This is true of all levels of healthcare. Putting the efficacy of HSCT or Alemtuzumab to one side, there is also the mental satisfaction / reward of 'nipping it in the bud' 'fighting hard' 'moving on'. In contrast, maintenance therapy's serve as a constant reminder that the disease is lurking and you're merely keeping it at bay. That is my own experience (on Ocrevus) and one of the reasons i am seeking out an IRT currently - the others being the higher efficacy, potential for improvements, impact on smouldering MS of course. The difficulty for patients is the point in the disease course at which these decisions need to be made in order to be most effective. I imagine a lot of patients who pursue HSCT are scared into it by a nasty relapse or as a last throw of the dice. Maybe less so with Alemtuzumab as it doesn't have the fatality cloud hanging over it or the hair loss, which seems to be a marker for something being seriously wrong. It is much easier to push these decisions down the road......take the risks if you need to but often then it is too late. Not easy.