


MMR vaccine: to vaccinate or not?
My mother has always been into alternative health, and as a result, I did not have an MMR vaccine as a child, nor did I have the HPV vaccine as a teenager. What should I do?

Case study
I am a 24-year-old woman with what I think is early relapsing-remitting MS. My first attack was mild optic neuritis when I was 19 and in my second year of University. I then developed a tight band around my chest in April this year, followed by numbness and pins and needles in my legs. I now know the band to be an episode of the so-called MS hug. I have just been diagnosed with MS and have been recommended to start Kesimpta (ofatumumab) as soon as possible. My mother has always been into alternative health, and as a result, I did not have an MMR vaccine as a child, nor did I have the HPV vaccine as a teenager. My current neurologist has suggested I speak to my GP about this. What do you recommend I do?

Prof G’s Opinion
Yes, and yes, you should have both vaccines.
Are you aware that ofatumumab being an anti-CD20 therapy blunts vaccine responses, particularly antibody responses to new vaccines or so-called neoantigens (new antigens)?
HPV vaccine
I have covered the topic of the HPV (human papillomavirus) vaccine in an earlier newsletter (Case study: cervical intraepithelial neoplasia (CIN) and ocrelizumab; 6-Nov-2021). Please read it.
The good news is that you can now receive the Gardasil-9 or polyvalent vaccine and get a broader cover than the Gardasil-4 or quadrivalent vaccine you should have received as a teenager. As you are less than 25 years of age, the NHS will cover the costs of the vaccine. I recommend having two doses of the vaccine before starting ofatumumab and the 3rd or booster dose sometime between months 6 and 12 after starting treatment.
MMR vaccine
The MMR vaccine is a live attenuated vaccine. Individuals 12 months or older should receive one dose, and a second dose should be given at least four weeks after the first dose. If you only received one dose of the MMR vaccine as a child, the NHS recommends getting a second booster dose (NHS recommendations on MMR vaccine); this also applies to adults.
I would recommend you have the two doses of the MMR vaccine and wait 3-4 weeks after the second dose before starting ofatumumab. You may be able to coordinate the first two doses of the HPV vaccine and MMR vaccines together to save time.
Other vaccines
At the same time, you should also have the pneumococcal vaccine and review your other childhood vaccines with your GP. You may need polio and diphtheria, tetanus and pertussis vaccines as well.
More on the MMR vaccine
I assume you know about Andrew Wakefield? Andre Wakefield proposed a causal association between the MMR vaccine and the subsequent development of autism. Despite Wakefield being discredited and being struck off the medical register in the UK, he and many other anti-vaxxers are still profoundly impacting society (see article below), which has filtered down to how we manage MS. Your case illustrates this.
The number of children receiving the vaccines in England is falling and is way below the WHO 95% threshold required for herd immunity. The downside is that we have seen epidemics of measles, yes measles, in the UK.
So what has this got to do with MS? Well, unvaccinated people also get MS. If you are unvaccinated, you are at risk of acquiring these infections as an adult. If you then go on to long-term immunosuppression to treat your MS, you are at risk of serious complications from these infections. In addition, once you are on long-term immunosuppressive therapy, you can’t necessarily be vaccinated; for example, the MMR vaccine as it is a live attenuated vaccine and is contraindicated if you are on immunosuppressive therapy.
If patients don’t have documentation of having had two doses of the MMR vaccine as a child, I screen them for immunity against all three viruses at baseline, i.e. before initiating a maintenance immunosuppressive therapy, to ensure they have immunity to MMR. If they are antibody negative, we offer them the option of receiving the MMR. Please be aware that individual component vaccines are not available in the UK at present.
My practice is not new. I know several other MS centres that also do MMR antibody screening.
My big concern for someone with MS on immunosuppressive therapy is to be exposed to measles and then develop measles inclusion-body encephalitis, which is usually fatal. This would be a particular problem for patients on natalizumab as this drug blocks the trafficking of T-cells into the CNS, which are required for antiviral responses.
As with all medical interventions, you can’t force people to have a vaccine, but it remains our responsibility to make sure pwMS have been given the option of being vaccinated and to provide evidence-based advice. One of the legacies of COVID-19 is that everyone is now vaccine-aware and has an opinion about the benefits and risks of vaccination. As an HCP, I am responsible for educating my patients and the wider community about the role of vaccination in preventing infections and the complications of these infections in vulnerable people. By doing this, we hopefully counter the anti-vaxx lobby, who are responsible for 100,000s of unnecessary deaths worldwide, not to mention the long-term sequelae of many of these preventable infections.
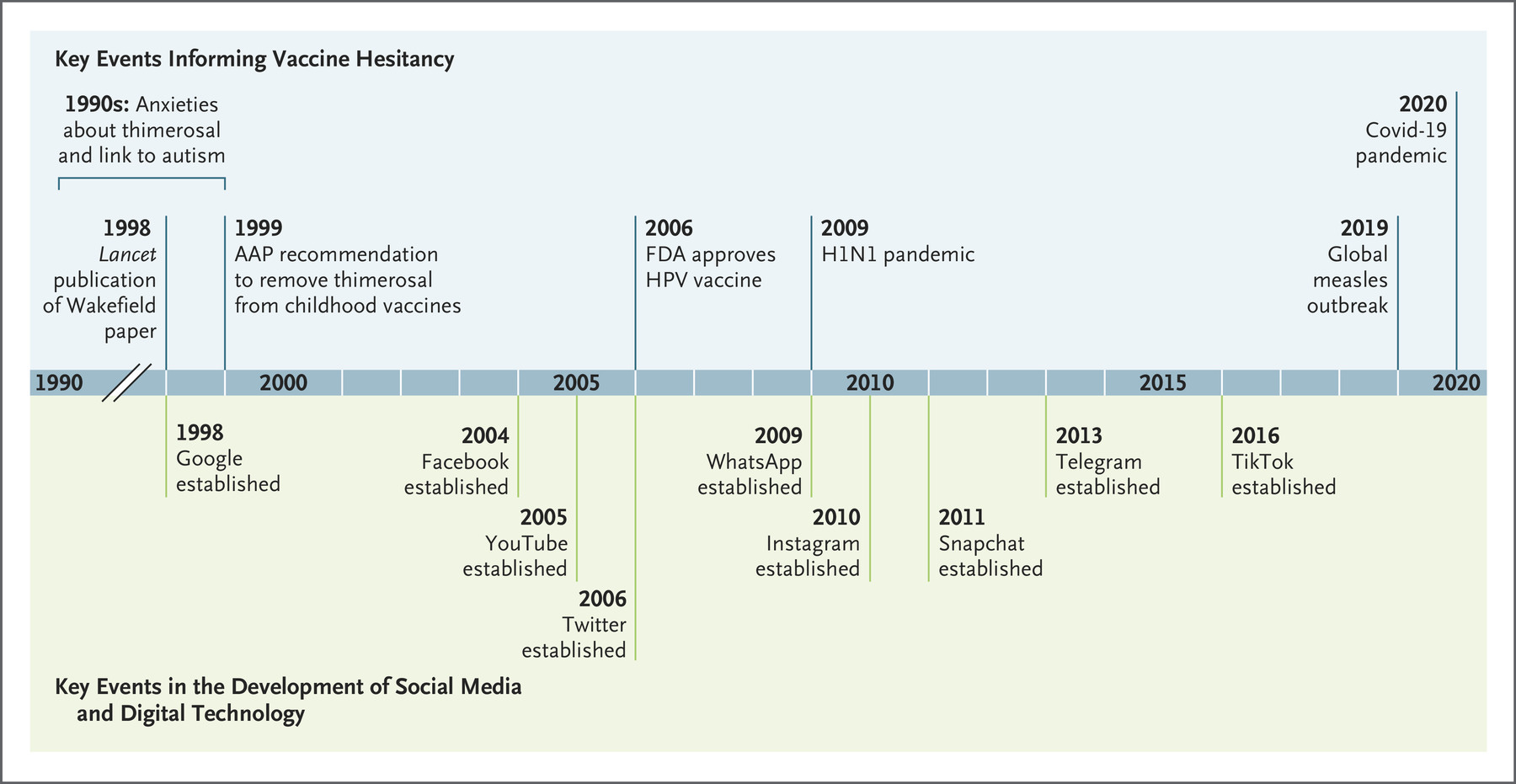
If you are interested in the issues around vaccine hesitancy, I suggest you read the following article from the NEJM.
Larson et al. The Vaccine-Hesitant Moment. N Engl J Med. 2022 Jul 7;387(1):58-65.
Subscriptions and donations
Paid subscriptions to MS-Selfie are being used to administer the Newsletter and associated MS-Selfie microsite currently in development. At the request of several readers, I have now added the option of making a one-off donation. To keep this initiative open to all readers, I would appreciate it if those who can afford a subscription, please subscribe. For active paying subscribers, thank you; your contribution is much appreciated.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry or Barts Health NHS Trust. The advice is intended as general advice and should not be interpreted as being personal clinical advice. If you have problems, please tell your healthcare professional who will be able to help you.
We had this with my son. My ex was an alternative health practitioner - but in Traditional Chinese Medicine (pins and herbs) and in TCM despite what everyone thinks, they really like their data and numbers. I work in IT but have previously worked in pharmacovigilance (drug safety). My ex was very concerned about the childhood vaccinations and possible risks from the vaccines. I wasn't yet on immune-suppression therapies but nonetheless wanted my kid to be vaccinated. So we "did our own research".
I showed her how to calculate the relative risks and relative benefits, where to find the relevant SPCs and trial data and we did massive spreadsheets working on risks. The numbers are pretty stark, I'll be honest. We didn't just look at "deaths" because just as important (or maybe even more important) are the life-long consequences. Autism lasts your whole life, as does brain damage, deafness etc.
We looked closely at the risk of permanent deafness / permanent brain damage from measles and the rest (but mainly measles, the others are milder) - and it was pretty obvious to her that our son should get his vaccinations, so he did.
The only one he didn't get, because why would he need THAT - was HepB.
He was 5 when I failed Tecfidera and was being offered Ocrevus, both he and his mother got the HepB vaccine to protect daddy :') - he was very brave (chocolate may have been involved in this bravery - but still very brave).
Whilst anecdotal evidence isn't evidence, he is a fit, healthy, fully bilingual (Spanish and English), very lovely* 8 year-old about 2 years ahead of himself in the school system here.
*I don't think being precocious / pesky is a known side effect of MMR / pentavac and therefore conclude it's inherited from his mother ;-)
I never understood what anyone had against vaccines: more specifically, vaccines to combat disease. I really don’t understand their distrust and mistrust of people who devote years of their lives to be educated, by thousands of other people who have devoted YEARS of their lives to the ONGOING and ever-expanding study of biology and medicine, that has been built on hundreds (if not a couple millennia) of years of experience, studies, trial and error, and teaching to others—as well as holding everyone else charged with the title of doctor to the same high standards by committee. These medications that have been created by many people working many hours, over many weeks or months or years, building on enormous amounts of previous information and experience, to help fight illnesses that harm is, hurt and kill.
I do understand the explanations, but they don’t comport with the reality of modern medicine. People say they don’t trust drug companies or the medical drug regulators. This is understandable from some of the news stories that circulate from time to time. But it’s not just those entities involved development and/or dissemination and/or guaranteeing safety and efficacy… it’s the whole medical community. And it’s based on everyone’s knowledge and intelligence in the community, not just one person or a few. And if you don’t trust that entire community, then you’ve got a real problem. A whole community of doctors can’t be a union of conspirators looking to fool us—can’t fool everyone all the time. I was once an assistant in a stem cell lab at the University of California, Irvine, and I was talking to a visiting doctor from CHOC (Children’s Hospital of Orange County), who was using the lab to study cerebral cancer specimens of children from around eighteen months to about eleven years old. A difficult job in many ways, as you might imagine. We were talking about the universe of people working on cures, and I asked him what he thought about the people who worked on cures and therapies only because the work interested them as a singular and insular pursuit, or just for the money, instead of because they really care about people and want to help them. He thought about it for a moment and then said, "You know Chris, there are a lot of us who do everything we possibly can to find cures and ease suffering because we want to help people, and even though we might not like it there are those who work on cures and therapies for selfish reasons, and have no interest in whether someone lives or dies. But actually we really need everyone." That was a good lesson for me, and probably a good lesson for anyone.