


Anti-CD20 therapies
A summary of the class of anti-CD20 therapies that includes ocrelizumab, ofatumumab, ublituximab and rituximab. Slow but steady progress in getting the MS-Selfie microsite done.

We launched the MS-Selfie Microsite at ECTRIMS in Milan. This is the final piece to complete the questions you must address before starting/switching to a multiple sclerosis (MS) disease-modifying therapy. I hope you find it helpful. I would appreciate any feedback to help the medical writing team when converting the information from the Newsletter to the microsite.
How do I want my MS to be treated? What is the difference between a maintenance/escalation DMT and an IRT (immune reconstitution therapy)?
How can I reduce my chances of adverse events on specific DMTs?
What are the attributes of the specific DMTs or treatment strategies?
Will I be able to become a parent? What about pregnancy and breastfeeding?
Anti-CD20
Summary
Anti-CD20 therapies are a class of monoclonal antibodies that bind to CD20 on the surface of B-cells. They work by depleting peripheral B-cells. Four anti-CD20 antibodies are available for treating MS and are administered by intravenous or subcutaneous injection. The three licensed agents for treating MS are ocrelizumab (Ocrevus), ofatumumab (Kesimpta) and ublituximab (Briumvi). All three of these agents are licensed for relapsing forms of MS, with only ocrelizumab having a license to treat primary progressive MS as well. Please note in many countries, rituximab (MabThera) is used off-label and will be increasingly so as it has recently been included on the WHO’s EML (essential medicines list) as a treatment for MS.
Most B-cell killing due to anti-CD20 is done through immunological processes that burst or lyse the cells, releasing their contents. This can cause a cell lysis syndrome or infusion reaction, which in the case of anti-CD20 therapies tends to be mild to moderate. The infusion reactions are typically managed by predosing with steroids, antihistamines and antipyretics (paracetamol/ acetaminophen or a non-steroid anti-inflammatory such as ibuprofen).
Ocrelizumab (600 mg), ublituximab (450 mg) and rituximab (1,000 mg) are given as 6-monthly intravenous infusions and ofatumumab (20mg) as monthly subcutaneous injections. However, the first dose of ocrelizumab is divided into two 300 mg doses two weeks apart, the first dose of ublituximab as 150 mg followed by 450 mg two weeks later and the first dose of rituximab as two 1,000 mg infusions two weeks apart. Ofatumumab is administered by subcutaneous injection with initial doses at weeks 0, 1 and 2, followed by subsequent monthly dosing starting at week 4.
The anti-CD20 therapies are highly effective DMT with a high rate of no evident inflammatory disease activity (NEIDA), slowing down disability worsening and brain volume loss. A recent real-world study suggests that ocrelizumab is more effective than rituximab. However, as these agents have yet to be compared head-to-head in a clinical trial, it is difficult to claim one is more or less effective than the others.
Rituximab and ublituximab are the least humanised and are associated with a higher rate of anti-drug (ADAs) and neutralising antibodies (NABs): 6.4% in ublituximab-treated subjects and is even higher in rituximab-treated patients. Between 1-2% of ocrelizumab-treated and less than 0.5% of ofatumumab-treated patients develop anti-drug antibodies as these are more humanised therapeutic antibodies and less likely to induce an anti-drug immune response. The ADAs and NABs are important considerations when choosing between these products.
The most common adverse effects are mild infusion-like reactions (generally not seen with subcutaneous ofatumumab), infections, low antibody levels in the blood (hypogammaglobulinaemia), blunted vaccine responses and rarely delayed neutropenia. In the ocrelizumab trials, there was an increased number of malignancies (including breast cancers), but the incidence was within the background rate expected for an MS population, and post-marketing studies have not shown an increased rate of malignancies.
Anti-CD20 therapies are generally available first-line to treat DMT-naive patients. As a class, anti-CD20 therapies have transformed the management of MS by allowing the adoption of a treatment strategy of using high-efficacy DMTs first-line, which I refer to as ‘flipping the pyramid’. Importantly, ocrelizumab has also ushered in the era in which we can treat PPMS.
Trade names
Kesimpta/Bonspri (ofatumumab): Kesimpta is sold in an autoinjector, and Bonspri as a vial for self-administration. Bonspri is only available in some middle and low-middle-income countries, where it is sold at a discount to Kesimpta.
Briumvi (ublituximab): ublituximab is the latest anti-CD20 therapy to be shown to be effective in MS and is not widely available yet.
MabThera (rituximab): please note rituximab is off-patent, and there are now a large number of biosimilars available across the world.
Mode of action
Anti-CD20 therapies work via peripheral B-cell depletion. It is unknown how B-cell depletion works as a treatment for MS. However, It is hypothesised that CD20 therapies work via several mechanisms involving the B-cell and possibly through a small population of CD20-expressing T-cells:
Preventing autoantigen presentation via the B-cell
Reducing B-cell-derived proinflammatory cytokines
Reducing B-cell production of autoantibodies
Depleting pro-inflammatory effector CD20-expressing T-cells
As an anti-EBV agent, EBV resides in memory B-cells, and depleting these cells decreases EBV viral loads. However, it is currently unknown what role EBV plays in the pathogenesis of MS.
Efficacy
High. Compared to active comparators (interferon-beta and teriflunomide), anti-CD20 therapies reduce the annual relapse rate by ~50% and three-month disability progression by a third. The no evident disease activity (NEDA) rates across two years of the pivotal trials are ~50%, and they slow down accelerated brain volume loss to ~0.3-0.4% per annum.
Class
Maintenance therapy - continuous B-cell depletion
Immunosuppression
Yes, long-term.
Dosing
Ocrevus (ocrelizumab): the initial 600 mg dose is administered as two separate intravenous infusions; first as a 300 mg infusion, followed two weeks later by a second 300 mg infusion. These initial infusions are given over 2.5 hours. Subsequent doses of ocrelizumab are administered as a single 600 mg intravenous infusion every six months. The infusion rate will vary from 2.0 to 3.5 hours, depending on how well it is tolerated. It is recommended that a minimum interval of 5 months should be maintained between each dose of ocrelizumab.
Kesimpta/Bonspri (ofatumumab): The recommended dose is 20 mg ofatumumab administered by subcutaneous injection with initial dosing at weeks 0, 1 and 2, followed by monthly dosing, starting at week 4.
Briumvi (ublituximab): the first dose is administered as a 150 mg intravenous infusion over four hours (first infusion), followed by a 450 mg intravenous infusion over one hour (second infusion) 2 weeks later. All subsequent doses are administered as a single 450 mg intravenous infusion every 24 weeks over an hour.
MabThera (rituximab): please note rituximab is off-patent, and there are now a large number of biosimilars available across the world. The most common dose is 1000 mg of intravenous rituximab on days 1 and 15 and then 1000 mg intravenously every six months. There are many variations to this dosing scheme, with many neurologists reducing the dose or extending the interval between doses to try and reduce the risk of long-term adverse effects.
Pre-treatment and prophylaxis treatment
For the anti-CD20 therapies, 100 mg of methylprednisolone (or an equivalent corticosteroid) is administered intravenously approximately 30 minutes before each infusion to reduce the frequency and severity of infusion reactions. This can be combined with chlorpheniramine 10 mg. Paracetamol 1g and/or ibuprofen 400mg PRN is given on an as-required basis for pyrexia, myalgias or pain, which can rarely occur as part of the infusion reaction. As the infusion reactions are only a problem with the first and second courses, many centres now omit methylprednisolone and antihistamines once patients are B-cell depleted and established on the treatment. The infusion reactions are due to a cell lysis syndrome. Once B-cell depletion is established, there are too few circulating B cells to cause a cell lysis syndrome. Prophylactic antivirals or antibiotics are not required with the anti-CD20 therapies.
Please note no premedication is not necessary with subcutaneous ofatumumab.
Off-label rituximab
Rituximab is off-patent and is relatively cheap, which explains why it is one of the drugs on the MS-Selfie off-label essential DMT list for treating MS in resource-poor environments. It is also worth noting that rituximab is one of three DMTs added to the WHO List of Essential Medicines to treat MS.
Main adverse events
Infusion-related reactions
Infusion-related reactions (IRR) are relatively common and experienced by about 1 in 3 subjects with the first and second infusions. Typical IRRs include pruritus, rash, urticaria, erythema, flushing, low blood pressure, pyrexia, fatigue, headache, dizziness, throat irritation, oropharyngeal pain, shortness of breath and throat or laryngeal swelling, nausea, tachycardia. The risk of anaphylaxis is very low.
Infection
Infections are the most common adverse event with anti-CD20 therapies. Infections tend to be minor. However, occasional severe infections occur. Respiratory tract infections are the most common reported infection. Herpes infections are also reported more frequently in anti-CD20 treated patients, including herpes zoster and oral and genital herpes simplex virus infection.
Laboratory abnormalities
Anti-CD20 treatment decreases total immunoglobulins, mainly driven by a reduction in IgM and IgA levels. Decreased levels of IgG tend to occur later and are associated with a higher risk of infection and severe infections. Not all patients treated with anti-CD20s develop hypogammaglobulinaemia.
A minority of pwMS treated with anti-CD20 therapies develop mild lymphopaenia. A small number of pwMS (<1%) develop grade 3 lymphopaenia (< 500 cells/mm3). An increased rate of serious infections has been seen during episodes of lymphopaenia.
A small number of anti-CD20 treated patients develop neutropaenia. The neutropaenia tends to be mild and transient, with less than 1% developing grade 3 (between 500 and 1000 cells/mm3) or grade 4 neutropaenia (< 500 cells/mm3). Please note neutropaenia can occur several months after starting anti-CD20 therapy and has been associated with infections.
To derisk infectious complications, we recommend all patients have a vaccine review and ensure they are up-to-date with their seasonal flu and COVID-19 vaccines. In addition to this, we recommend all patients have the pneumococcal (Pneumovax) and the VZV (Shingrex) vaccines before starting anti-CD20 therapy (please see ‘Derisking DMTs’, 20-Aug-2022). Some pwMS may want to consider additional vaccines before starting an anti-CD20 therapy.
As anti-CD20 therapies are immunosuppressive, they increase the likelihood of infections. To derisk infections, we recommend routine baseline screening for HIV, syphilis, hepatitis B and C and tuberculosis. In addition, we screen for exposure to VZV, and if seronegative, we strongly recommend getting the VZV vaccination before starting therapy.
Malignancy
An increased number of malignancies (including breast cancer) were seen in ocrelizumab-treated subjects in clinical trials. However, the incidence appears to be within the background rate expected for an MS population. Patients must follow standard breast cancer screening guidelines, i.e. monthly self-examination and women between 50 and 70 years of age should have mammograms every 3 years. Other potential cancers linked to anti-CD20 therapies include basal cell carcinoma.
Pharmacovigilance monitoring requirements
Baseline
Full blood count, urea and electrolytes, liver function tests, thyroid function tests, serum immunoglobulin levels, serology (varicella-zoster virus, human immunodeficiency virus 1 and 2, hepatitis B and C, TB ELISpot, up-to-date cervical smear and/or human papillomavirus testing, a pregnancy test and baseline blood pressure are done.
Follow-up
No routine follow-up blood tests are mandated. However, we now monitor the full blood count and serum immunoglobulin levels every 6-12 months when patients come in for their infusions or annual follow-up appointments. The latter is particularly relevant for patients on subcutaneous ofatumumab.
Rebaselining
A rebaseline MRI scan needs to be done after starting an anti-CD20 therapy. I recommend that an MRI is done at ~6 months after starting treatment and that Gd-enhancement is ideally included as part of the rebaselining MRI. A monitoring MRI is then done annually after that (resources permitting).
Women of childbearing potential and pregnancy
The SmPc recommends that women of childbearing should use contraception while receiving anti-CD20 and, in the case of ocrelizumab, for up to 12 months after the last infusion. I tend to ignore this requirement in women who want to start or extend their families. I give such women the option of starting an anti-CD20 and falling pregnant in their own time. Most women don’t fall pregnant immediately; it takes, on average, four ovulation cycles to fall pregnant and often much longer than this. Ocrelizumab doesn’t affect fertility and is not teratogenic (affects the developing baby). In addition, the placenta only matures towards the end of the second trimester when it allows antibodies (anti-CD20 is an antibody) to cross from the maternal circulation into the developing baby's circulation. So once a woman falls pregnant, we delay the next infusion until after the baby's delivery. Even if small amounts of ocrelizumab cross over into the baby’s circulation, it tends to cause a transient B-cell depletion in the baby.
Breastfeeding
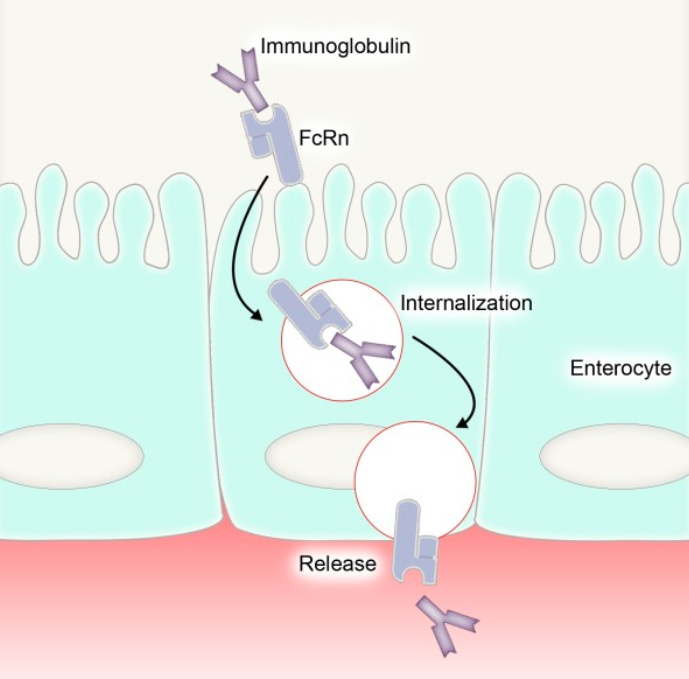
In general, monoclonal antibodies, including the anti-CD20 therapies, are safe during breastfeeding as little gets into the breast milk, and the small amounts that do get into the breast milk will be metabolised in the baby’s gastrointestinal tract. The exception is in the first 2-3 weeks post-partum when a woman’s breasts produce colostrum, and the newborn’s intestinal tract is immature and can transfer antibodies across the intestinal surface.
Colostrum, or first milk, is produced immediately after the newborn's delivery and for about 2-3 weeks after delivery. Colostrum is exceptionally high in antibodies and other factors to protect the newborn against disease and infection. As the newborn’s gastrointestinal tract is immature, many of the proteins in colostrum are absorbed and will have systemic immune effects.
Most of the antibodies in colostrum are IgA and IgM produced by plasma cells in the breast. Therefore, I suspect that circulating IgG, including ocrelizumab, will only get transferred into breast milk in small amounts. However, the breast epithelial cells express the so-called neonatal Fc-receptor, the molecular shuttle for transporting antibodies into milk. In addition, this neonatal Fc receptor shuttle is also expressed in the newborn intestine. So, the molecular mechanisms are in place to potentially increase your developing baby’s exposure to ocrelizumab.
So, if you plan to breastfeed, which I recommend, you would want to avoid ocrelizumab when your breasts produce colostrum. There are no black-and-white answers to any problem in MS. Delaying recommencing ocrelizumab treatment for a few weeks post-partum outweighs the chances of rebound disease activity.
Fertility
Animal studies and experience in humans reveal no issues concerning fertility.
Vaccination
It is recommended that anti-CD20 treated patients are immune to the varicella-zoster virus (VZV) before starting treatment. Patients should also be offered the pneumococcal (Pneumovax) and VZV (Shingrex) component vaccines to boost immunity before treatment. Antibody response to neoantigens (new vaccines) is blunted in patients on anti-CD20 vaccines, not T-cell responses. Therefore, patients on anti-CD20 therapies can have inactivated vaccines and mount a partial response to the vaccine. Live attenuated vaccines are not recommended to patients on anti-CD20 therapies.
Travel
People with MS need to be aware that being on an anti-CD20 may affect travel; for example, some countries require you to be vaccinated against yellow fever, which is a live attenuated vaccine. Therefore, the yellow fever vaccine must be given before starting anti-CD20.
High versus low dose anti-CD20
To move our treatment target in MS beyond NEIDA (no evident inflammatory disease activity), the new focus has to be on preventing end-organ damage and the processes driving smouldering MS, i.e. stopping disability progression, normalising brain volume loss, flattening the area under the neurofilament level curve, stopping slowly expanding lesions from getting bigger, clearing the CSF of oligoclonal IgG bands and if possible promoting repair and recovery of the nervous system.
What good is it to be free of relapses and focal MRI activity if you get worse? This is why the concept of using low-dose anti-CD20 therapy seems flawed. Trial participants exposed to lower doses of ocrelizumab in the phase 3 trials, due to body size, do as well as those exposed to higher doses in relation to relapses and MRI activity, but not in relation to worsening disability or smouldering disease.
The phase 3 ocrelizumab trials used a fixed dose of 600mg of ocrelizumab intravenously every 6 months. By doing this, smaller pwMS got a larger dose of ocrelizumab than larger people. For example, someone weighing 60 kg got 10mg/kg of ocrelizumab 6-monthly compared to 5mg/kg for someone with MS weighing 120 kg. Trial subjects could be divided into four groups or quartiles representing four dosing levels by measuring drug concentrations. Despite no difference between these four groups concerning the treatment effect of ocrelizumab on relapses and MRI activity, those subjects who received higher doses and had more significant B-cell depletion were less likely to progress. This higher-dose treatment effect on smouldering MS, i.e. beyond NEIDA, was seen in both the relapsing and primary progressive populations.

From these post-hoc analyses of the phase 3 ocrelizumab trials, it is clear that you may need higher, and not lower, doses of anti-CD20 therapy to tackle smouldering MS. At the moment, these observations only apply to the initial two years of treatment. Hence, we don’t know if pwMS will only need higher doses as an induction strategy to purge the various B-cell compartments of pathogenic (disease-causing) cells.
Once you have purged these compartments after two years of high-dose anti-CD20 treatment, you may not need to maintain pwMS on such high doses of anti-CD20 therapy, which will continue suppressing normal B-cell biology and immune responses with long-term complications. There are two large phase 3 trials testing high-dose ocrelizumab (1200 and 1800mg every 6 months) to standard-dose ocrelizumab (600mg every 6 months) in both relapsing and primary progressive MS. The results of these trials will hopefully answer some of the lingering questions about dosing anti-CD20 therapies.
Please note that lower dose anti-CD20 therapies are a moving target and should not be equated with peripheral B-cell counts, which are a poor surrogate for what is happening in the deep tissues and CNS. We need better and more accessible biomarkers to study these compartments. Receiving ocrelizumab less than the licensed 6-monthly dose, rituximab, ofatumumab or ublituximab could potentially be classified as low-dose anti-CD20 therapy.
Summary of Product Characteristics (SmPC)
Switching to an anti-CD20 therapy
Interferon and glatiramer acetate
An anti-CD20 therapy can be started immediately after discontinuing interferon-beta or glatiramer acetate. All the recommended baseline screening tests and vaccination reviews must be done before starting one of the anti-CD20s.
Natalizumab
Owing to the risk of rebound activity on stopping natalizumab, a prolonged wash-out period is not recommended. Most often, the reason for switching from natalizumab to an anti-CD20 or another DMT is to reduce the risk of carry-over PML (progressive multifocal leukoencephalopathy) from natalizumab. In our centre, we do an MRI and a lumbar puncture for cerebrospinal fluid analysis to exclude JC virus-DNA on polymerase chain reaction testing. Provided these two tests are clear, we typically initiate the anti-CD20 after the last natalizumab infusion as soon as possible. All the recommended baseline screening tests and vaccination reviews must be done before starting an anti-CD20.
S1P modulators (fingolimod, siponimod, ozanimod and ponesimod)
Because fingolimod has quite a long half-life, some neurologists recommend a short washout period, i.e. 4 ̶- 6 weeks; this may be appropriate, depending on the reason for switching. I recommend waiting for the total peripheral lymphocyte counts to exceed 800/mm3 to exclude the uncommon occurrence of lymphopaenia following S1P modulator administration. All the recommended baseline screening tests and vaccination reviews must be done before starting an anti-CD20. If you are switching because of abnormal liver function tests on an S1P modulator, you would ideally want the liver enzymes to normalise or at least drop to below three times the upper limit of normal before starting an anti-CD20.
Fumarates
All the recommended baseline screening tests and vaccination reviews must be done before starting an anti-CD20. If lymphopaenia is the main reason for switching from fumarate, I recommend waiting for the total peripheral lymphocyte counts to exceed 800/mm3 before starting an anti-CD20.
Teriflunomide
All the recommended baseline screening tests and vaccination reviews must be done before starting an anti-CD20. I recommend that the total peripheral lymphocyte counts are above 800/mm3 before starting an anti-CD20. We don’t routinely do an accelerated washout of teriflunomide before starting an anti-CD20.
Anti-CD20 therapies (selective cell depleting DMTs)
If patients switch between formulations of anti-CD20 therapies out of choice (patient preference), it can be done without safety concerns and needing to wait for B-cell counts to recover. If patients are switching for loss of efficacy, I suggest checking for anti-drug antibodies and reviewing the diagnosis of MS to try and understand why the particular patient has not responded to the specific anti-CD20 and/or its formulation.
Mitoxantrone/Alemtuzumab/Cladribine/AHSCT
Before starting an anti-CD20 therapy, I recommend waiting for the neutrophil and total peripheral lymphocyte counts to go above 1,000/mm3 and 800/mm3, respectively. An exception to this would be the cases of severe rebound that are rarely seen after alemtuzumab. In these circumstances, the anti-CD20 therapy is given to treat very active, often pseudotumoral, MS. All the recommended baseline screening tests must be done before starting an anti-CD20 therapy.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. You must be a paying subscriber if people want to ask questions unrelated to the Newsletters or Podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
X (Twitter) / LinkedIn / Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.
Another possible question: How long can I stay on a DMT - is there an age limit?
Off topic - i dont know where to post otherwise- i live in Wales and had more than 5 relapses in a year in 2020. Ive been dx 2021 and been on tysabri since shortly after even though my jcv titre was 3.10 from the beginning.
Can someone tell me how to get hsct because my ms nurses keep saying it's not available in Wales.
Thabk you