
Cladribine
Cladribine is a selective immune reconstitution therapy (IRT) and is the only IRT on the WHO List of Essential Medicines for treating multiple sclerosis.

I am almost there. We will be officially launching the MS-Selfie Microsite at ECTRIMS in Milan. Before we can launch, I need to complete the list of questions I have put together to help people with MS make an informed decision about starting a disease-modifying therapy and have all the newsletters transferred onto the microsite. This newsletter is a draft of the information you need to know about cladribine.
I would appreciate any feedback to help the medical writing team when converting the information from the Newsletter to the microsite.
How do I want my MS to be treated? What is the difference between a maintenance/escalation DMT and an IRT (immune reconstitution therapy)?
How can I reduce my chances of adverse events on specific DMTs?
What are the attributes of the specific DMTs or treatment strategies?
Will I be able to become a parent? What about pregnancy and breastfeeding?
Cladribine
Summary
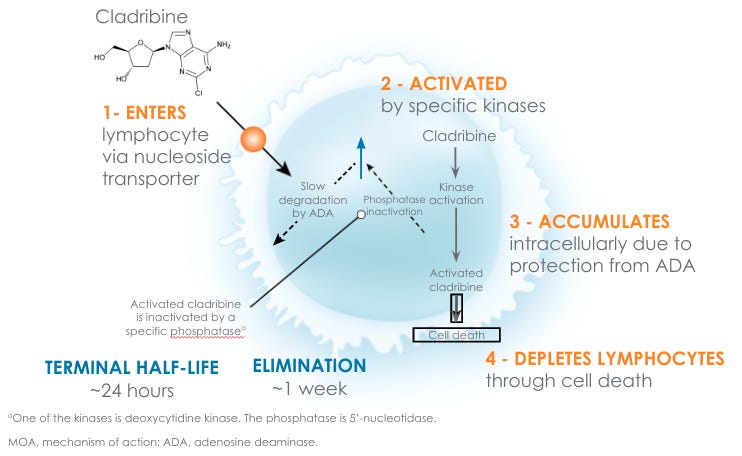
Cladribine is a small molecule drug belonging to a class called purine analogues. Cladribine’s chemical name is 2-chloro-2'-deoxyadenosine [2-CdA]. Cladribine is inactive, but once inside a cell, it is activated by adding three phosphate groups by an enzyme called deoxycytidine kinase (DCK). In its triphosphoylated state, it is incorporated into DNA, which then blocks further extension of the DNA chain by the so-called DNA polymerases. The failure to be able to extend or repair DNA is sensed by the cell, which triggers the cell to die by a process called programmed cell death or apoptosis. When cells die by apoptosis, they don’t release their contents via cell lysis but are gradually taken up by cells of the reticuloendothelial system by phagocytosis. This is why lymphocyte cell death occurs slowly after cladribine administration, and there is no cell lysis syndrome. This explains why cladribine-treated patients with MS don’t get infusion-type reactions, nor do they need steroids and antihistamines to prevent these reactions.
Cladribine is selective in mainly targeting lymphocytes, particularly B-lymphocytes, because DCK, the enzyme that activates cladribine, is expressed in high levels in these cells.
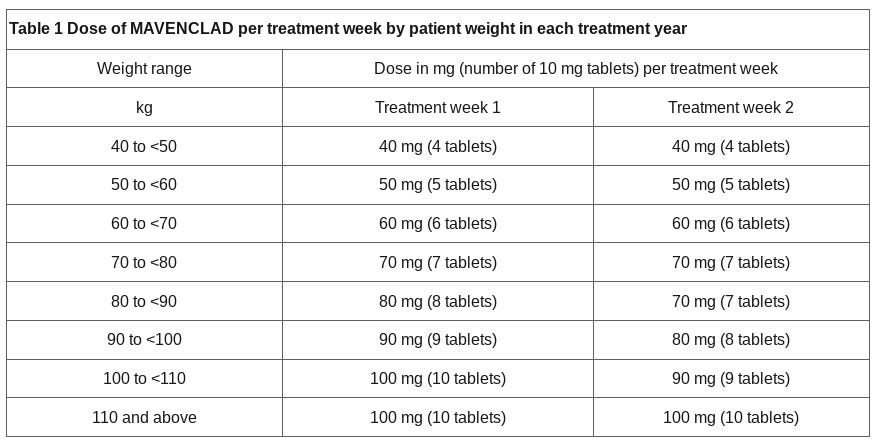
Cladribine is given as two courses of oral tablets with a recommended cumulative dose of 3.5 mg/kg body weight over two years. Each treatment course consists of 2 treatment weeks, one at the beginning of the first month and one at the beginning of the second month of the respective treatment year. The treatment course in year two can be delayed to six months if the lymphocyte counts have not recovered above 800/mm3. Each treatment week consists of 4 or 5 days on which a patient receives 10 or 20 mg (one or two tablets) daily.
Cladribine works by depleting your lymphocytes and then allowing them to recover over several months. It is an immune reconstitution therapy (IRT); hence, after your immune system recovers, hopefully without the cells that cause MS, it can fight infections, respond to vaccines and provide peripheral immune surveillance for tumours.
Cladribine is a highly effective DMT with a high rate of no evident inflammatory disease activity and slows down disability worsening. Cladribine is very well tolerated, with almost no side effects after taking the tablets. The most common adverse effects are infections, which tend to be mild. A minority of patients can experience a non-specific headache after taking cladribine. No delayed secondary autoimmunity is seen after cladribine, differentiating it from alemtuzumab and AHSCT, two other IRTs used to treat MS.
Contrary to the label, cladribine is unlikely to be associated with a higher risk of secondary malignancies. Many patients treated with cladribine go into long-term remission with no evident inflammatory disease activity. Whether these individuals are cured or not will require much longer follow-up. Claribine works similarly to alemtuzumab (Lemtrada) or AHSCT (autologous haemopoietic stem cell transplantation) but is a much safer treatment option.
Trade name
Mavenclad
Mode of action
Cladribine or 2-chloro-2'-deoxyadenosine [2-CdA] is a purine analogue. Cladribine is taken up by cells via specific transporter proteins. Cladribine is inactive, but once inside a cell, it is activated by adding three phosphate groups by an enzyme called deoxycytidine kinase (DCK). In its triphosphoylated state, it is incorporated into DNA, which then blocks further extension of the DNA chain by the so-called DNA polymerases. The failure to be able to extend or repair DNA is sensed by the cell, which triggers the cell to die by a process called programmed cell death or apoptosis. Cells that die by apoptosis don’t release their contents via cell lysis but are gradually taken up by cells of the reticuloendothelial system by phagocytosis. This is why lymphocyte cell death occurs slowly after cladribine administration, and there is no cell lysis syndrome. This explains why cladribine-treated patients with MS don’t get infusion-type reactions, nor do they need steroids and antihistamines to prevent these reactions.
A group of enzymes called the 5'-nucleotidases (5’-NT) can dephosphorylate activated cladribine. Purines and purine analogues are usually broken down by an enzyme called adenosine deaminase (ADA), but cladribine is relatively resistant to breakdown by ADA. The ratio of DCK:5’-NT, which is very high in lymphocytes compared to other cell types, and cladribine’s resistance to being metabolised by ADA explains why cladribine selectively targets lymphocytes, particularly B-lymphocytes, and not other cells. Interestingly, when it comes to lymphocytes, B-cells are more sensitive to cladribine than T-cells, i.e. they are depleted to a greater extent, and cells from the innate immune system are relatively resistant to the effects of cladribine. This unique depletion pattern, particularly memory B-cells, explains why cladribine-treated patients are not at high risk of opportunistic or common bacterial infections and why cladribine-treated patients are not at increased risk of delayed secondary autoimmunity.
Like IRTs, cladribine treatment aims to kill the cells that cause MS or reset regulatory mechanisms that keep the autoreactive cells under control when the immune system recovers. As an IRT, cladribine works by rebooting the immune system.
Efficacy
High. Compared to placebo, cladribine reduced the annual relapse rate by nearly 60% and three-month disability progression by a third. The NEDA rates across the two years of the pivotal trial were close to 50%, and cladribine did slow down accelerated brain volume loss by ~0.56% per annum. The impact on brain volume loss was more pronounced in patients with clinically isolated syndrome (<0.2% per annum), indicating that cladribine’s effect is greatest when used early. Cladribine is licensed in the UK as a therapy for people naive to treatment with rapidly evolving severe MS or as a second or third-line therapy for people with highly active MS.
A minority of patients treated with cladribine go into long-term remission with no evident inflammatory disease activity. In a long-term follow-up study of subjects from the pivotal phase 2 trials population, over 50% of study subjects had not started another DMT 13+ years after last being exposed to cladribine, indicating a long-term treatment effect of cladribine. Whether some of these individuals are cured or not requires much longer follow-up. Cladribine works similarly to alemtuzumab and AHSCT (autologous haemopoietic stem cell transplantation) but is a much safer treatment option. Cladribine is CNS penetrant with levels in the spinal fluid ~25% of those in the blood, which is at a level for cladribine to have a treatment effect in CNS-resident lymphocytes.
Class
Selective immune reconstitution therapy
Immunosuppression
Yes, short-term, whilst the immune system is depleted. The immune system is competent once reconstitution occurs, typically 6 to 9 months after treatment.
Dosing
Cladribine is given as two courses of oral tablets with a recommended cumulative dose of 3.5 mg/kg body weight over two years, i.e. 1.75 mg/kg per year. Each treatment course consists of 2 treatment weeks, one at the beginning of the first month and one at the beginning of the second month of the respective treatment year. The treatment course in year two can be delayed to six months if the lymphocyte counts have not recovered above 800/mm3. Each treatment week consists of 4 or 5 days on which a patient receives 10 or 20 mg (one or two tablets) daily.
Following completion of the two treatment courses, no further cladribine treatment is required in subsequent years unless there is a recrudescence of disease activity. Additional courses are given if breakthrough activity occurs later on. Although the label states that no treatment is required in years 3 and 4, retreatment can be safely given with a similar safety profile to the initial two courses. The problem with retreatment in years 3 and 4 relates mainly to reimbursement of the drug as it is licensed as a treatment for a period of 4 years. In many countries, Merck, the manufacturer of Mavenclad, will provide the drug for free in years 3 and 4.
Table 1 - Dose of cladribine per treatment week by patient weight in each treatment year
Recurrent MS disease activity
If you have recurrent disease activity in year one after the first course, we can bring the second course forward by 3-4 months, provided your total lymphocyte count has recovered to 800/mm3. Breakthrough disease activity in year one occurs in about one in ten patients. This does not necessarily mean cladribine has failed you, but you need the second course to get on top of your MS disease activity. Disease breakthrough in year two after the second course of cladribine, particularly if associated with poor depletion of lymphocytes, is considered a treatment failure. Poor depletion of lymphocytes occurs in a very small number of pwMS (<2-3% of treated subjects) and likely indicates resistance to the mode of action of cladribine.
As with other IRTs, recurrent MS disease activity after year two does not necessarily mean cladribine has failed you. It is simply an indication for retreatment, i.e. giving a third or fourth course of cladribine. Please note that under the NHS England treatment algorithm, we only have permission to administer additional courses after year 4. Please note that if someone has breakthrough MS disease activity after cladribine, there is no reason any other MS DMT cannot be started, provided all the baseline tests are done for that DMT before starting the treatment.
Pre-treatment and prophylaxis treatment
Importantly, no pretreatment or prophylactic antivirals or antibiotics are required to prevent infusion reactions or infections with cladribine, respectively. This differentiates cladribine from the other IRTs, i.e. mitoxantrone, alemtuzumab and AHSCT.
Parenteral cladribine
It is worth pointing out that oncologists have used intravenous and subcutaneous cladribine for decades to treat a rare type of leukaemia called hairy cell leukaemia and some types of lymphoma. Therefore, some units offer off-label parenteral cladribine to treat MS. Parenteral cladribine is off-patent and is relatively cheap, which explains why it is one of the drugs on the MS-Selfie off-label essential DMT list for treating MS in resource-poor environments. It is also worth noting that cladribine is one of three DMTs added to the WHO List of Essential Medicines.
Main adverse events
The most common clinically significant adverse event reported with cladribine is herpes zoster due to the varicella-zoster virus (VZV) reactivation. The risk of zoster was higher in association with grade 3 or 4 lymphopenia (<500/mm³). Please note grade 3 or 4 lymphopaenia was most common in year two after the second course and tended to occur in subjects who received their second course before their lymphocyte counts had recovered to above 800/mm3 after the first course. Delaying the second course of cladribine until the lymphocyte count recovers to above 800/mm3 means grade 3 and 4 is less common, and hence zoster is less common. In addition to this, the Shingrex vaccine is now recommended to all patients before starting immunosuppressive therapies to boost immunity to VZV and further lower the risk of developing zoster (please see ‘Derisking DMTs’, 20-Aug-2022).
As cladribine is an immunosuppressive therapy, it may increase the likelihood of infections. To derisk infections, we recommend routine baseline screening for HIV, syphilis, hepatitis B and C and tuberculosis. In addition, we screen for exposure to VZV, and if seronegative, we recommend getting the VZV vaccination before starting cladribine. Because the T-lymphocytes are only partially depleted by cladribine, leaving behind sufficient numbers to protect you from opportunistic infections, which are very uncommon in cladribine-treated pwMS. For example, to my knowledge, there has not been a case of progressive multifocal leukoencephalopathy (PML) in cladribine-treated pwMS. You will notice in Mavenclad SmPC that cladribine is associated with a higher incidence of cancers. With time, this risk has dissipated as more data has been collected. Therefore, I don’t think cladribine is associated with a secondary malignancy risk.
When we completed the phase 3 CLARITY trial (two doses of oral cladribine vs. placebo in relapsing forms of MS), there was an imbalance in cancers, which resulted in an obvious cancer signal. Four subjects developed cancers in the two treatment arms, compared to no cancers in the placebo arm, i.e., a two to zero ratio (Giovannoni et al. N Engl J Med. 2010 Feb 4;362(5):416-26.). There will always be a signal when you have zero in the denominator. This is why the regulators include cancer as a risk in the Mavenclad label and why it is part of a black-box warning in the USA.
However, over time, new data has emerged to suggest the risk is not an obvious signal, at least in the short- to intermediate-term. The types of cancers we saw in the CLARITY trial are not those associated with immunosuppression. There was a case each of breast cancer, pancreatic cancer, melanoma and choriocarcinoma of the uterus. Apart from choriocarcinoma, derived from the placenta and pregnancy-related, the other three cancers probably take years to evolve and are likely to have been developing before cladribine exposure. The typical cancers you see with immunosuppression are basal and squamous cell cancers of the skin and lymphomas. We haven’t seen excess numbers of these types of cancers in cladribine-treated pwMS, which is reassuring.
When my colleagues then looked at the cancer rate in cladribine-treated subjects in the trial, they found it to be very similar to the cancer rates associated with other MS disease-modifying therapies (Pakpoor et al. Neurol Neuroimmunol Neuroinflamm. 2015 Oct 1;2(6):e158.). The cancer rate, however, was abnormally low in the placebo-treated arm of the CLARITY trial. I, therefore, think the apparent cancer signal in the trial was driven by the low rate in the placebo arm and not a high rate in the treatment arm. The cancer signal would not have been there if we had just one cancer in the trial's placebo arm.
Another clue is when we followed up with the placebo-treated patients after the phase 3 trials; they had a higher rate in the subsequent years than in the subjects in the active treatment arms exposed to cladribine in the first two years. This suggests the placebo-treated subjects didn’t develop their cancers in the trial but did so afterwards; this type of lag-time bias can happen by chance.
We then compared the cancer rate in the cladribine-treated patients to what is expected in the general population. To do this, we compare the rates in cladribine-exposed patients to the cancer rate in the global cancer registry. By doing this, you get a standardised incidence rate or SIR that is very close to one, i.e. the expected cancer rate. Over time, the SIR has remained close to one (no increased risk), but more importantly, the confidence intervals around this value have become very small or narrow. This makes it highly likely that no cancer signal is associated with cladribine treatment.
Finally, contrary to what many people think, cladribine is not a mutagen. Although it works through DNA mechanisms by triggering apoptosis or cell death, it does not cause direct mutations in DNA. The correct term for a drug like this is a clastogen. I suspect the legacy of cladribine has been determined by its repurposing from oncology; therefore, it is assumed by inference to be a mutagen and must damage DNA and work as a cytotoxic therapy. In reality, cladribine’s mode of action is very nuanced, and it is not a cytotoxic therapy. Cladribine gradually causes cell apoptosis over weeks to months and is not associated with cell lysis syndrome.
Another clue to the cladribine cancer signal being a false-positive comes from the oncology registers of patients who have received cladribine and related drugs for hairy cell and chronic lymphoid leukaemia. There was no increased cancer signal in this register despite these patients being much older than people with MS treated with cladribine (Cheson et al. J Clin Oncol. 1999 Aug;17(8):2454-60.).
Although the Mavenclad SmPC states cladribine is contraindicated in pwMS with active malignancies, the decision is much more nuanced than this, and an individual benefit-risk evaluation should be performed before initiating cladribine. Because cladribine is an IRT with only moderate short-term immunosuppression, it provides an advantage in some patients with prior malignancy. It puts MS in remission and allows normal immune function after immune reconstitution. Please note that all cladribine-treated pwMS should be advised to follow standard cancer screening guidelines, which differ from country to country.
Less common adverse events after cladribine include liver toxicity, rash, hypersensitivity reactions, hair loss and neutropaenia.
Pharmacovigilance monitoring requirements
Baseline
Full blood count, urea and electrolytes, liver function tests, thyroid function tests, serum immunoglobulin levels, serology (varicella-zoster virus, human immunodeficiency virus 1 and 2, hepatitis B and C, TB ELISpot, up-to-date cervical smear and/or human papillomavirus testing, a pregnancy test and baseline blood pressure are done.
Follow-up
Lymphocyte counts should be determined before initiating the second course of cladribine in year two. A full blood count and liver function tests are done 2 and 6 months after each treatment year start. If the lymphocyte count is below 500 cells/mm³, some neurologists use antiviral prophylaxis and actively monitor lymphocyte counts until they increase again. This is not my practice, as the onset of zoster is not always synchronized with the period of lymphopaenia. Because you don’t treat cladribine-induced lymphopaenia, there is little point in monitoring lymphocyte counts frequently. Cladribine-treated patients are told to be vigilant for any clinical signs and/or symptoms such as unexplained bleeding, bruising, nausea, vomiting, abdominal pain, fatigue, loss of appetite, jaundice and/or dark urine and a temperature or other symptoms of an infection. As with all immunosuppressive therapies, it is essential to detect infections early to treat them promptly.
Rebaselining
A rebaseline MRI scan needs to be done after caldribine. I recommend that an MRI is done between 18-24 months after starting treatment and that Gd-enhancement is included as part of the rebaselining MRI. A monitoring MRI is then done annually after that.
Women of childbearing potential and pregnancy
If you are a woman of childbearing age, we require a negative urine pregnancy test before starting cladribine infusions. Cladribine is potentially teratogenic, i.e. it may cause birth defects. We don’t advise patients to fall pregnant or father a child until at least six months after the last exposure to cladribine. However, in the case of an unplanned pregnancy in the so-called at-risk period, we would not recommend a termination of pregnancy. Cladribine has a short half-life and is undetectable after a week of dosing; hence, the foetus may not be exposed to active drug. We, therefore, refer patients to the high-risk pregnancy clinic for close monitoring. Ideally, women with MS should delay falling pregnant until after they have completed their second course of cladribine. If a woman falls pregnant before the second course, we delay the second course until after delivery, and the woman has stopped breastfeeding.
Breastfeeding
We don’t recommend cladribine whilst breastfeeding. It is a small molecule and will cross over into the breast milk. We advise pregnant women to wait until ten days after the last exposure to cladribine before breastfeeding again.
Fertility
There is no evidence that cladribine affects either male or female fertility. In animal studies, cladribine did not affect male fertility but transiently decreased sperm counts. This is why we recommend that male-treated patients wait until six months after completing a course of cladribine before trying to father a child.
Vaccination
It is recommended that cladribine patients are immune to the varicella-zoster virus (VZV) before treatment. Patients should also be offered the Shingrex component vaccine to boost immunity to VZV before treatment. There is no reason why cladribine patients can’t receive component or inactivated vaccines. However, the use of live attenuated vaccines may carry a risk of infections and – based on the current recommendation – should be avoided whilst immunosuppressed. However, once patients have reconstituted their immune function, they can receive live vaccines safely. The latter is one of the advantages of cladribine and other IRTs.
Travel
People with MS need to be aware that being on cladribine may affect travel; for example, some countries require you to be vaccinated against yellow fever, a live attenuated vaccine. Therefore, the yellow fever vaccine must be given before starting cladribine or after immune reconstitution.
Summary of Product Characteristics (SmPC)
Switching-2-cladribine
Interferon and glatiramer acetate
Cladribine can generally be started immediately after discontinuing interferon or glatiramer acetate. All the recommended baseline screening tests and vaccination reviews must be done before starting cladribine.
Natalizumab
A prolonged wash-out period is not recommended due to the risk of rebound activity on stopping natalizumab. Most often, the reason for switching from natalizumab to cladribine or another DMT is to reduce the risk of carry-over PML (progressive multifocal leukoencephalopathy) from natalizumab. In our centre, we have done an MRI and, in some patients, a lumbar puncture for cerebrospinal fluid analysis to exclude JC virus-DNA on polymerase chain reaction testing. Provided the MRI and CSF are clear, we would typically initiate cladribine after the last natalizumab infusion as soon as possible. All the recommended baseline screening tests and vaccination reviews must be done before starting cladribine.
S1P modulators (fingolimod, siponimod, ozanimod and ponesimod)
Because fingolimod has quite a long half-life, some neurologists recommend a short washout period, i.e. 4 ̶ 6 weeks; this may be appropriate, depending on the reason for switching. I recommend waiting for the total peripheral lymphocyte counts to exceed 800/mm3 to exclude the uncommon occurrence of persistent lymphopaenia following S1P modulator administration. All the recommended baseline screening tests and vaccination reviews must be done before starting cladribine. If you are switching because of abnormal liver function tests on an S1P modulator, you would ideally want the liver enzymes to normalise or at least drop to below three times the upper limit of normal before starting cladribine.
Fumarates
All the recommended baseline screening tests and vaccination reviews must be done before starting cladribine. If lymphopaenia is the main reason for switching from fumarate, I recommend waiting for the total peripheral lymphocyte counts to exceed 800/mm3 before starting cladribine.
Teriflunomide
All the recommended baseline screening tests and vaccination reviews must be done before starting cladribine. Before starting cladribine, I recommend the total peripheral lymphocyte counts above 800/mm3. We don’t routinely do an accelerated washout of teriflunomide before starting cladribine.
Anti-CD20 therapies (selective cell depleting DMTs)
All the recommended baseline screening tests and vaccination reviews must be done before starting cladribine. If patients are switching for safety concerns, they should wait for B-cell counts to recover before starting cladribine. If patients are switching for loss of efficacy on an anti-CD20, there is no need to wait for B-cell recovery.
Mitoxantrone/Alemtuzumab/AHSCT
I recommend waiting for the neutrophil and total peripheral lymphocyte counts to go above 1,000/mm3 and 800/mm3, respectively. All the recommended baseline screening tests must be done before starting cladribine.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. You must be a paying subscriber if you ask questions unrelated to the Newsletters or Podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your own healthcare professional, who will be able to help you.
Email comment: "I am extremely impressed by this. The level of detail is really high but still understandable, and this is something that is hard to find anywhere. I am a GP and would have loved to have this level of detail when making a decision about medications last November when I had a severe spinal cord relapse. I am wondering if you have a similar set of information about Ofatumamab?"
This is so great and thorough, I would have loved this when cladribine was proposed for me. I did my first two years, then needed to take a third year/set of doses in January 2022, and I have not looked back. I cannot tell you how “good” I’ve felt in the last 6 months, almost “normal”. I still have all my usual symptoms, but nothing worse. Reading about the mechanism of how it works, and details on its efficacy are so reassuring. You are changing the future of MS Dr Giovannoni, thank you.