

I was at the MS Trust conference this week. I ran a seminar on MDTs (multi-disciplinary team) meetings for MS-related DMTs (disease-modifying therapies) and gave a talk in the final plenary session on smouldering MS. If you want, you can download my talks from my slide share site. Please feel free to hack the presentations and use them as you want.

Building an effective MDT: roles, responsibilities, and ructions
The MDT session went very well. It was decided that what we are talking about is not an MDT, in the way the term should be used, but an MDM or multi-decision-maker meeting. In reality, these meetings are about disease-modifying therapies (DMTs) and not the overall management of MS. Most participants felt the term MDT should refer to meetings about the care of patients with complex needs and true MDTs should include a wider group of specialists, i.e. neurologists, therapists (physio, occupational and speech & language), nurses, continence, palliative care, community workers, psychologists, dietician, social workers, etc.
Smouldering multiple sclerosis: the ‘real multiple sclerosis’
My talk on ‘Smouldering MS’ in the final plenary session went down rather less well or even poorly. First, it was in the graveyard session before the close of the meeting when most delegates had already departed. Secondly, I was grilled by one of the delegates about using the term smouldering MS, which they and their team did not like, because the smouldering MS concept challenges decades of MS dogma around the treatment of MS. One of the points this delegate raised is that discussing smouldering MS, and downplaying the importance of relapses and focal MRI, is harmful to patients and conveys a negative picture of MS. She implied that it undoes the progress we have made in the field of MS. Do you agree?
My argument about decades of MS dogma is that science and data should win the day. If decades of MS dogma are wrong, ignoring new data and insights won’t make the old dogma less wrong. This is how science works; Thomas Kuhn wrote about it in his now-famous book “The Structure of Scientific Revolutions”. Kuhn argued that science and knowledge don’t develop by accumulating accepted facts and theories but by an episodic model in which periods of conceptual continuity (current dogma) are interrupted by periods of revolutionary science. The discovery of "anomalies" during scientific revolutions leads to new paradigms, which question and challenge old data and provide a new direction for future research.
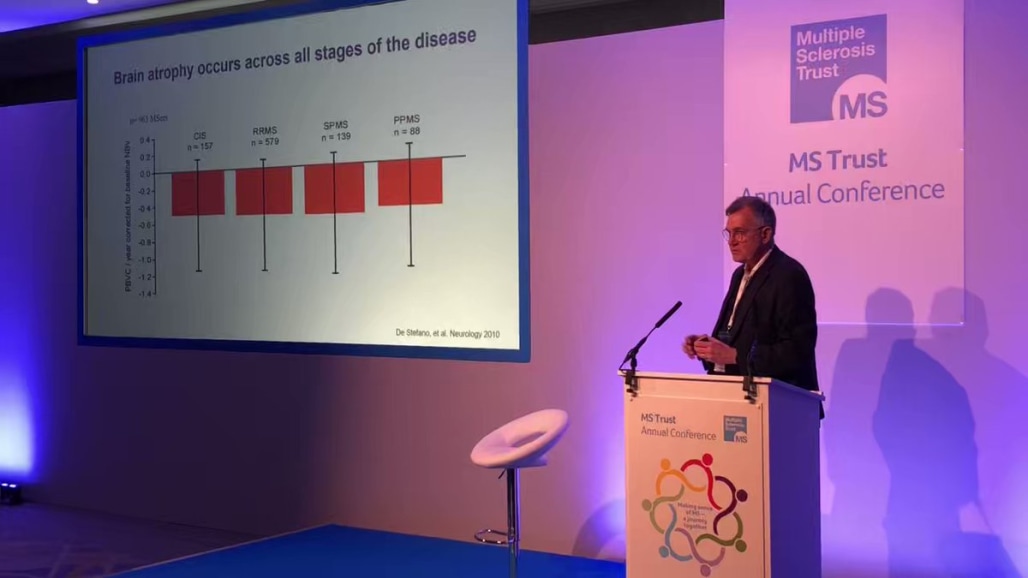
The concept of smouldering MS, focusing on the end-organ (brain and spinal cord), and showing that relapses and focal MRI activity are not MS is just such a revolution. Sadly, most of what I am talking about Professor George Ebers was saying in the mid to late 90s. If we continue to ignore the anomalies in the current model of MS, we won’t find the cause and cure for MS, and more importantly, we won’t develop the next generation of therapies for MS that will prevent, slow down or reverse smouldering disease.
Another thing is I strongly believe in treating people with MS as adults in the room. I tend not to pull my punches. PwMS would rather know the truth about their disease than have the wool pulled over their eyes. Telling someone with MS who complains of getting worse that their MS is stable and under control, because they are not relapsing or developing new lesions on MRI is a form of medical gaslighting. This is why I have argued for HCPs working in MS to understand these evolving concepts, assimilate them into their current thinking, develop a narrative to describe smouldering MS and focus on the things that can improve MS outcomes. The latter refers to my philosophy of marginal gains. Smouldering MS is not an untreatable condition; things can always be done to improve MS outcomes and the quality of life of pwMS.
I told the audience that the MS community is getting behind the concept of smouldering MS and that the pharmaceutical industry is developing new classes of therapies to tackle this aspect of the disease. BTK inhibitors are one class of therapy that targets both CNS resident B-cells and microglia (innate immune activation) in MS. Similarly, our Sizomus trial (ClinicalTrials.gov Identifier: NCT03783416) is testing a CNS penetrant next-generation proteasome inhibitor (ixazomib) to try and scrub the CNS of plasma cells. Antiviral therapies are another class of treatment targeting smouldering MS. Then there is exercise, diet, sleep, comorbidities, infections, antiageing strategies, modifiable social determinants of health, wellness, etc. So rather than being downbeat about smouldering MS, we need to be upbeat and celebrate the gains we have made with our anti-inflammatory DMTs and that we now have new targets and treatments to explore.
MS-Selfie microsite

Finally, the MS Trust conference was the event we chose to launch our MS-Selfie microsite. I spent a lot of time talking to attendees at the conference about MS-Selfie and what we are trying to achieve with the MS Self-Management revolution. Most attendees I spoke to had not heard of MS-Selfie, which means we have a lot of work to do to spread the word.
Subscriptions and donations
Paid subscriptions to MS-Selfie are being used to administer the Newsletter and associated MS-Selfie microsite, which is now open to all readers. At the request of several readers, I have now added the option of making a one-off donation. To keep this initiative open to all readers, I would appreciate it if those who can afford a subscription to subscribe. For active paying subscribers, thank you; your contribution is much appreciated. Because of the falloff in paying subscribers, I am considering returning to a paywall that will give paying subscribers six months of unlimited access to all newsletters. At the same time, free subscribers will have a wait to access the newsletters later, not as an email, but on the substack site.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your own healthcare professional, who will be able to help you.









Prof G chastised for discussing the real MS