



Case study
I saw a 46-year-old man with MS today in my clinic who has secondary progressive MS and is on siponimod (Mayzent). He has previously been failed by interferon-beta and fingolimod, and despite being on siponimod, he continues to notice a gradual worsening of his walking and early involvement of his right hand with loss of dexterity; he is having difficulty doing delicate motor tasks involving both hands (bimanual tasks). He questioned whether or not siponimod was working, considering he had been on fingolimod in the past. He also asked if MS could ever burn itself out.

Prof G’s Advice
Fingolimod to Siponinmod Switching
I previously wrote about switching from fingolimod to siponimod (please see ‘Managing smouldering MS’, 30-Aug-2021). The case for changing from fingolimod to siponimod is based on the evidence that siponimod has been shown to impact SPMS. Although both fingolimod and siponimod are S1P-modulators, siponimod is an active drug with more significant activity within the CNS on the so-called S1P-5 receptor that is expressed in oligodendrocytes and astrocytes. The latter is likely to be responsible for the effects of siponimod on the brains of people with SPMS, i.e. it slows down brain volume loss, in particular, grey matter volume loss, and siponimod-treated study subjects had improved tissue integrity on MRI and slower loss of cognition compared to placebo-treated subjects. In comparison, fingolimod did not impact brain volume loss in patients with primary progressive MS.
It is important to note that Siponimod is an active drug, and fingolimod is a pro-drug and needs to be activated or phosphorylated to work. The activation process, or variable activation, may explain why fingolimod has a different effect on the central nervous system when compared to siponimod.
Another reason for offering a switch from fingolimod to siponimod is to spread hope. It says that although you have secondary progressive MS, options are still available to slow down smouldering-associated worsening (SAW). The one obvious problem with the fingolimod to siponimod switch is that it means officially labelling you as having SPMS. This means, at least under the NHS, is not eligible to switch back to another DMT. Being labelled as having SPMS is a cul-de-sac.
The good news is that NHS England now allows us to switch patients from one DMT, such as fingolimod, to siponimod without having to have so-called ‘active SPMS’, i.e. having to have a recent history of relapse or new lesions on MRI. They now classify pwMS on a DMT with smouldering MS as having active SPMS. The rationale is that these patients do not have relapses or MRI activity because their current DMT suppresses focal inflammation. This new change does away with the perverse situation of having to stop a DMT and wait for the patient with SPMS to relapse and/or develop new lesions on MRI before becoming eligible for siponimod.
Burnt-out MS
Before writing this section, I thought I would ask ChatGPT if MS ever burns itself out. This is what I got back.
“Multiple sclerosis (MS) does not burn itself out. It is a chronic and lifelong condition that requires ongoing management and treatment. MS is an autoimmune disease where the immune system mistakenly attacks the protective covering of nerve fibers in the central nervous system. This leads to various symptoms such as fatigue, difficulty walking, numbness or tingling, muscle weakness, and problems with coordination and balance.” ChatGPT3
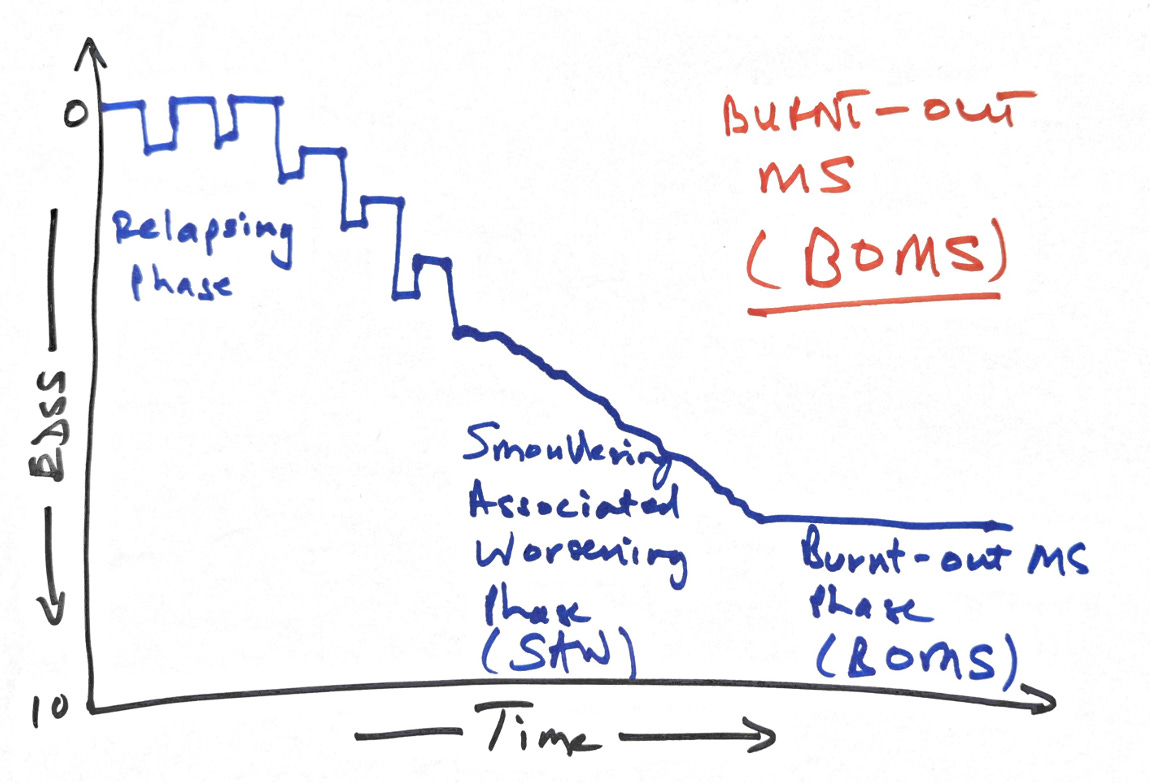
Professor WI (Ian) McDonald always pointed out that in his experience, a minority of patients with progressive MS would continue to worsen for several years. Then they would stop getting worse as if their disease burnt itself out. He used to tell his patients this in his clinic, claiming that about 1 in 10 patients or 10%, would develop this. He referred to this as a burnt-out MS (BOMS).
I know that burnt-out MS is a controversial topic, with not much in the literature. Many commentators mix up the concept of BOMS with benign MS. By definition, ‘benign MS’ is having MS for an extended period of time with little or no disability. In comparison, BOMS is flat-lining regarding disability worsening after a period of smouldering-associated worsening (SAW).
I agree with Prof. McDonald’s observation with the one proviso that many patients with BOMS, who may be stable for decades, often come back when they get older with deterioration in function likely to be age-related worsening. These patients tend to be in their 60s and 70s, and when you interrogate them with sensitive biomarkers, you find no evidence of MS disease activity.
The flatlining after a period of SAW may be therapeutic lag, i.e. it takes time for the anti-inflammatory effect of treatment to manifest as it takes time for the damage from past activity to manifest. In addition, some of the pathologies that underpin smouldering MS may also burn out with time.
For example, paramagnetic iron-rimmed lesions on MRI (PRLs), which are thought to expand slowly over time, may stop expanding after several years. In the study below, these lesions evolve, stop expanding and may even lose their iron rims. This is good news for pwMS in that smouldering MS may be modifiable and new treatments, for example, the BTK inhibitors, may prevent or reduce the rate of worsening and eventually lead to what is called BOMS. At least BOMS until ageing kicks in and further worsening is noticed.
I would be interested to know if you have heard about burnt-out MS or BOMS before and if any of you think you may have burnt-out MS.
For those new to MS-Selfie, I suggest reading ‘Getting Worse’ (02-July-2021). It is probably the most important MS-Seflie Newsletter I have written. In it, I explain why people with MS get worse. I will now update it to include a detailed discussion on BOMS.
Paper
Recent data suggest that multiple sclerosis white matter lesions surrounded by a rim of iron containing microglia, termed iron rim lesions, signify patients with more severe disease course and a propensity to develop progressive multiple sclerosis. So far, however, little is known regarding the dynamics of iron rim lesions over long-time follow-up. In a prospective longitudinal cohort study in 33 patients (17 females; 30 relapsing-remitting, three secondary progressive multiple sclerosis; median age 36.6 years (18.6-62.6), we characterized the evolution of iron rim lesions by MRI at 7 T with annual scanning. The longest follow-up was 7 years in a subgroup of eight patients. Median and mean observation period were 1 (0-7) and 2.9 (±2.6) years, respectively. Images were acquired using a fluid-attenuated inversion recovery sequence fused with iron-sensitive MRI phase data, termed FLAIR-SWI, as well as a magnetization prepared two rapid acquisition gradient echoes, termed MP2RAGE. Volumes and T1 relaxation times of lesions with and without iron rims were assessed by manual segmentation. The pathological substrates of periplaque signal changes outside the iron rims were corroborated by targeted histological analysis on 17 post-mortem cases (10 females; two relapsing-remitting, 13 secondary progressive and two primary progressive multiple sclerosis; median age 66 years (34-88), four of them with available post-mortem 7 T MRI data. We observed 16 nascent iron rim lesions, which mainly formed in relapsing-remitting multiple sclerosis. Iron rim lesion fraction was significantly higher in relapsing-remitting than progressive disease (17.8 versus 7.2%; P < 0.001). In secondary progressive multiple sclerosis only, iron rim lesions showed significantly different volume dynamics (P < 0.034) compared with non-rim lesions, which significantly shrank with time in both relapsing-remitting (P < 0.001) and secondary progressive multiple sclerosis (P < 0.004). The iron rims themselves gradually diminished with time (P < 0.008). Compared with relapsing-remitting multiple sclerosis, iron rim lesions in secondary progressive multiple sclerosis were significantly more destructive than non-iron rim lesions (P < 0.001), reflected by prolonged lesional T1 relaxation times and by progressively increasing changes ascribed to secondary axonal degeneration in the periplaque white matter. Our study for the first time shows that chronic active lesions in multiple sclerosis patients evolve over many years after their initial formation. The dynamics of iron rim lesions thus provide one explanation for progressive brain damage and disability accrual in patients. Their systematic recording might become useful as a tool for predicting disease progression and monitoring treatment in progressive multiple sclerosis.
Subscriptions and donations
Paid subscriptions to MS-Selfie are being used to administer the Newsletter and associated MS-Selfie microsite, which is now open to all readers. At the request of several readers, I have now added the option of making a one-off donation. To keep this initiative open to all readers, I would appreciate it if those who can afford a subscription to subscribe. For active paying subscribers, thank you; your contribution is much appreciated. Because of the falloff in paying subscribers, I am considering returning to a paywall that will give paying subscribers six months of unlimited access to all newsletters. At the same time, free subscribers will have a wait to access the newsletters later, not as an email, but on the substack site.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.









Share this post