



I was referred to a patient from another centre as he had relocated to East London. He had had multiple sclerosis (MS) for over 20 years and was interferon-beta-1a (Avonex). He was pretty disabled (EDSS 5.5), with an unsteady gait, lower leg weakness, slurred speech and cognitive impairment. He needed a walking aid but was determined to get by without one. He was divorced and lived alone. He had a teenage son who he rarely saw. He was unkempt and needed help. I was concerned about falls and his ability to look after himself. We arranged for a community nurse to do a home visit. She reported that his tiny one-bedroom apartment was overflowing with items, such as old packaging and items this patient had been collecting. She described narrow corridors between the piles of rubbish, which were at head height. His chair in front of the television, the TV, his bed, and his bathroom were connected by corridors walled with piles of clutter. His kitchen was so full of items that he could barely use it to prepare food. As a result of this, he mainly ate out or got takeaways. This pwMS had a hoarding disorder (HD), which I suspect was related to his MS.

Hoarding disorder (HD)
Hoarding is abnormal. People with HD are classified as having a mental health condition characterised by persistent difficulty discarding possessions that are not related to their value. Individuals with HD form an emotional attachment to their possessions. They often describe the items they have hoarded as having sentimental value, providing a sense of security, or they serve as reminders of past events.
Beyond the emotional components associated with hoarding, HD is also related to other cognitive difficulties, which include emotional dysregulation, poor executive functioning and problems with impulse control, attention, organisation and problem-solving. These mental issues contribute to the excessive accumulation of clutter, a defining feature of HD. While HD can theoretically affect anyone, it is particularly prevalent among older adults. It is estimated that more than one in 20 people over the age of 70 has HD. On reflection, I have seen many people with MS display some features with HD. I know about it as community teams often do home visits and have to clear the homes of disabled people before adjustments can be made so they can cope with their disabilities. I have never thought much of it, but I suspect it may be more common than expected in pwMS. I would like to know if you are a hoarder or have HD.
People with HD tend to be older and have physical limitations, which may hinder their ability to manage clutter. Clutter creates safety issues related to tripping and falling, poses a fire hazard, and can obstruct access in an emergency. In one of my patients, another older man, the paramedics couldn’t get a stretcher into a home because of the clutter.
A recent US Senate report highlights a crisis stemming from the rising prevalence of hoarding disorder (HD), particularly amongst the ageing population and, in my experience, pwMS and other neurodegenerative disorders. The US HD report stresses the significant health and safety risks, including increased fire hazards, and advocates for a coordinated national response.
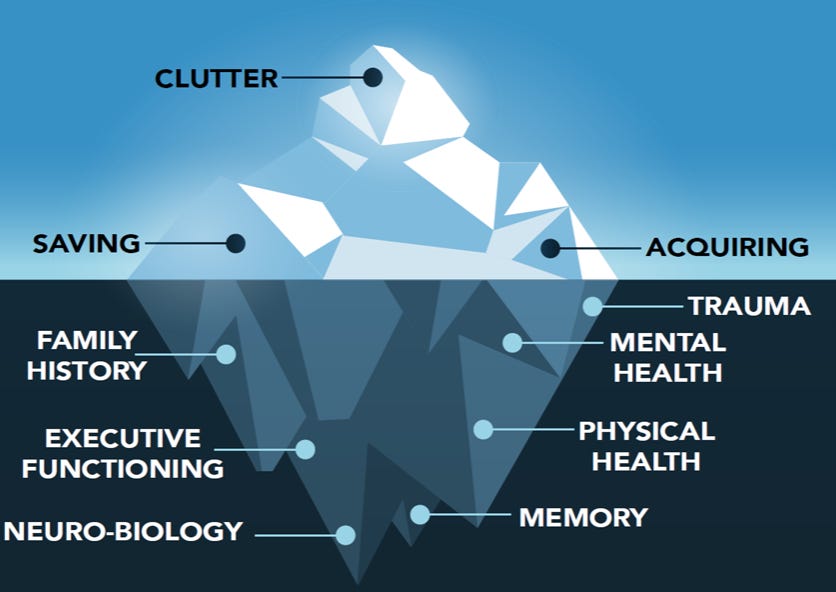
HD is classified as one of the obsessive-compulsive disorders (OCD) and is more common in people with OCD. As with most psychiatric diagnoses, the primary symptom or sign, as in the case of hoarding, typically represents the tip of an iceberg with many hidden symptoms (see figure below).
At present, effective treatments for HD are limited, primarily focusing on cognitive behavioural therapy (CBT). Some new approaches, such as virtual reality and cognitive rehabilitation, may help.
The following are the diagnostic criteria for primary HD under DSM-5.
Disorder Class: Obsessive-Compulsive and Related Disorders
Persistent difficulty discarding or parting with possessions, regardless of their actual value.
This difficulty is due to a perceived need to save the items and the distress associated with discarding them.
The difficulty of discarding possessions results in the accumulation of possessions that congest and clutter active living areas and substantially compromise their intended use. If living areas are uncluttered, it is only because of the interventions of third parties (e.g., family members, cleaners, or the authorities).
The hoarding causes clinically significant distress or impairment in social, occupational, or other important areas of functioning (including maintaining a safe environment for oneself or others).
The hoarding is not attributable to another medical condition (e.g., brain injury, cerebrovascular disease, Prader-Willi syndrome).
The hoarding is not better explained by the symptoms of another mental disorder (e.g., obsessions in obsessive-compulsive disorder, decreased energy in major depressive disorder, delusions in schizophrenia or another psychotic disorder, cognitive defects in major neurocognitive disorder, restricted interests in autism spectrum disorder).
Specify if:
With excessive acquisition: If difficulty discarding possessions is accompanied by excessive acquisition of items that are not needed or for which there is no available space. (Approximately 80 to 90 percent of individuals with hoarding disorder display this trait.)
Specify if:
With good or fair insight: The individual recognises that hoarding-related beliefs and behaviours (pertaining to difficulty discarding items, clutter, or excessive acquisition) are problematic.
With poor insight: The individual is mostly convinced that hoarding-related beliefs and behaviours (pertaining to difficulty discarding items, clutter, or excessive acquisition) are not problematic despite evidence to the contrary.
With absent insight/delusional beliefs: The individual is completely convinced that hoarding-related beliefs and behaviours (pertaining to difficulty discarding items, clutter, or excessive acquisition) are not problematic despite evidence to the contrary.
Survey
I would be interested to know if any of you were aware of the possible association between hoarding and MS and if any of you display some of the traits of HD or have been diagnosed and treated for HD. I would therefore appreciate it if you could complete this short survey on MS and hoarding. It will take you less than 5 minutes.

Thanks.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. You must be a paying subscriber if people want to ask questions unrelated to the Newsletters or Podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.








Share this post