



I have just returned from a lecture tour of Canada, which included four cities in four days and 12 speaking arrangements. My host's hospitality and kindness were exceptional. Thank you, thank you. I felt appreciated.
I have previously done lecture tours of Canada, Australia, and India. People, including my wife, often ask why I accept these invitations, as they are gruelling. I suspect it is flattery, i.e., it is nice that people still want to hear you talk even when you are in the twilight of your career and dodging bullets in snipers' alley. Yes, I have just had my second melanoma excised, and I am waiting for the histology report. The period of not knowing a result that could have significant implications for your management is what you must go through every year you have a monitoring MRI. It is anxiety-inducing.
The other side of travel and lecture tours is thinking and feedback time. When you get away from the Toads, you have time to test new ideas and revisit old ideas and concepts with a critical audience. The Canadian audiences asked difficult questions. All of this helps refine your thinking.
Please note that Toads references the late Philip Larkin’s poem about work (it is one of my favourites). Whilst away, you also get time to read new literature and listen to new things without being distracted by Toads.

Toads, by Philip Larkin (March 1954)
Why should I let the toad work
Squat on my life?
Can't I use my wit as a pitchfork
And drive the brute off?
Six days of the week it soils
With its sickening poison -
Just for paying a few bills!
That's out of proportion.
Lots of folk live on their wits:
Lecturers, lispers,
Losers, loblolly-men, louts-
They don't end as paupers;
Lots of folk live up lanes
With fires in a bucket,
Eat windfalls and tinned sardines-
They seem to like it.
Their nippers have got bare feet,
Their unspeakable wives
Are skinny as whippets - and yet
No one actually _starves_.
Ah, were I courageous enough
To shout, Stuff your pension!
But I know, all too well, that's the stuff
That dreams are made on:
For something sufficiently toad-like
Squats in me, too;
Its hunkers are heavy as hard luck,
And cold as snow,
And will never allow me to blarney
My way of getting
The fame and the girl and the money
All at one sitting.
I don't say, one bodies the other
One's spiritual truth;
But I do say it's hard to lose either,
When you have both.
Canada
Before I started the tour, Canadian neurologists were asked what they wanted to hear me speak about. The themes were:
The new MS McDonald criteria: what I thought of them and how their implementation would change MS practice.
Emerging challenges in the management of MS: I focused on making MS one disease and targeting smouldering MS.
Ageing and MS: Does late-onset MS differ from young-onset MS, and how does age affect MS management? Interestingly, this is the one talk I never delivered.
EBV and MS prevention: This is closest to my current research interest.
You can download them from my file-sharing site to read, hack, and use the slides in your talks. Many years ago, I realised that my job as an academic is creating and disseminating knowledge. Knowledge creation is your research output, and dissemination is communicating your findings via conferences, publications, lectures, blogs, podcasts, patents or teaching. To help disseminate knowledge, I share my slides with anyone who wants to read and learn from them. I don’t mind people hacking my slides for their talks; please proceed. And if you disagree with them, let me know!
EBV immunotherapies
Many Canadian neurologists asked about using EBV-targeted immunotherapy to treat MS. The discussion revolved around the recent failure of Atara Bio's allogeneic cytotoxic T-cell therapy, Moderna’s EBV therapeutic vaccine trial, which will be starting soon, and B-cell and EBV-targeted CAR T-cell therapies.
In MS, the T-cell response to EBV is exhausted, particularly the CD8+ cytotoxic T-cells (CTL) response, which leads to poor virus control. This is why, in pwMS, EBV is often found to be cycling through its latent and lytic infection cycles. This latent-lytic-cycling is at the core of the driver hypothesis of how EBV causes MS. We and others have proposed to use EBV-targeted immunotherapy as a treatment for MS. The adoptive transfer of in vitro-expanded autologous EBV-specific CD8+ T cells directed against viral latent proteins was shown to work in a proof-of-concept study by Michael Pender’s group. This approach was then explored using the adoptive transfer of partially MHC-matched allogenic EBV-specific T-cells (Atara Bio). However, the phase 2 EMBOLD trial of ATA188 in non-active progressive multiple sclerosis was negative. I have discussed this trial on many occasions on MS-Selfie. Whether this trial failed because of the poor survival of these allogeneic cells is unknown. Other possibilities include poor trial design, i.e. targeting people with too advanced MS and severe disability, and expecting a read-out within 12 months was unrealistic. Another factor is the product itself. How good was it compared to freshly prepared autologous cells?
Moderna’s approach will use an EBV RNA vaccine to boost the immune responses to EBV. Many centres in Canada are participating in this trial, and our centre at Barts Health has also put up its hand. My problem with the Moderna approach is that if the immune system of pwMS sees EBV all the time, i.e., from latent-lytic cycling, why will a vaccine work? Will the vaccine sufficiently wake the EBV-specific T-cells from their senescing slumber? I have hypothesised that the vaccine will not be potent enough to achieve its aims. What is needed is to reverse the T-cell exhaustion or senescence that characterises MS-associated T-cell responses. Agents that do this in cancer are called immune checkpoint inhibitors (ICI). A therapeutic EBV vaccine may need an ICI to boost T-cell responses, which will then control EBV and MS disease activity. Moderna know about this strategy as their latest therapeutic melanoma vaccine is being tested with pembrolizumab (Keytruda), the biggest selling ICI.
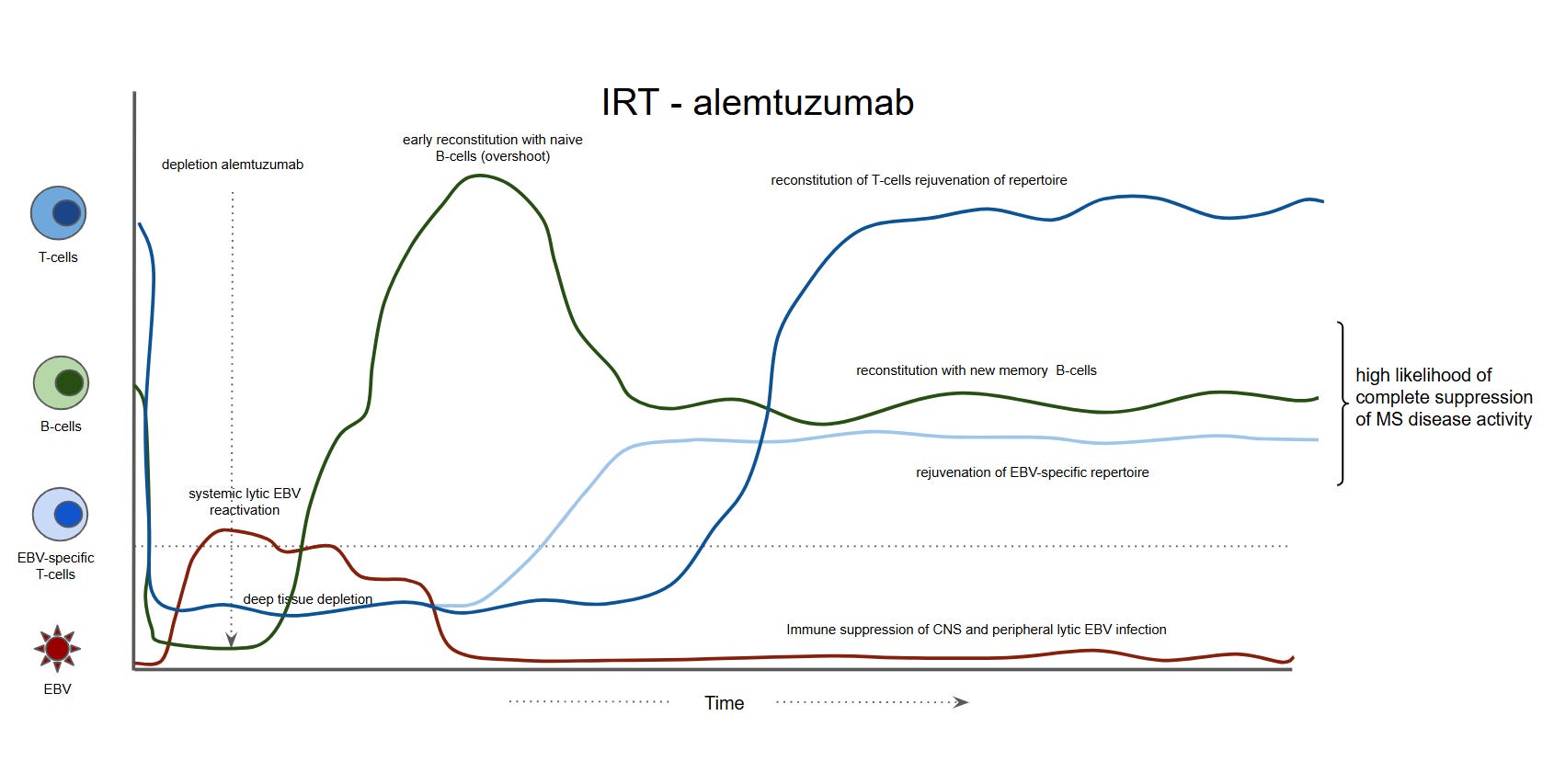
In support of this is the observation that IRT (immune reconstitution therapies) such as autologous haematopoietic stem cell transplantation (AHSCT) or alemtuzumab may be working like this already. The depletion cycle of both AHSCT and alemtuzumab has a paradoxical effect, resulting in EBV reactivation as T-cell and NK-cell function is impaired. However, when NK-cells and T-cells repopulate, they are rejuvenated and provide an effective EBV-specific T-cell response, which enables them to control EBV. Notably, almost all MS patients undergoing AHSCT have EBV viraemia detected in the peripheral blood, which supports this mechanism.
Many Canadian neurologists queried my suggestion about using an ICI in pwMS. However, contrary to current dogma, pwMS with comorbid cancer seem to tolerate ICIs without obvious recrudescence of MS disease activity. This observation is a powerful argument against MS being a T-cell-mediated autoimmune disease. The CNS demyelination cases triggered by ICIs appear to be ADEM and not MS, which makes sense as ADEM is a T-cell-mediated disease. ADEM is the human equivalent of EAE (experimental allergic encephalomyelitis), the main animal model of MS, which is primarily driven by T-cells.

The obvious question from these observations is whether ICIs could be used as a monotherapy to treat MS. Do we need an EBV therapeutic vaccine at all; can’t we rely on endogenous EBV to trigger autoimmunity? I suggest Moderna take a step back and do a small proof-of-concept study looking at the EBV-specific immune responses that their vaccine induces in a small number of pwMS. If they don’t overcome the T-cell exhaustion, they could test their vaccine in combination with an ICI to ensure it works immunologically before doing a costly phase 2 trial. But who am I to pontificate about what will and won’t work in MS in relation to the EBV hypothesis?
Another thing that resurfaced in my consciousness is that if EBV causes MS, it has to explain everything about the disease. For example, AHSCT and alemtuzumab have such a dramatic effect on stopping the end-organ damage that is occurring in MS, as neither of these treatments has direct CNS effects. The T-cell rejuvenation and EBV autovaccine hypothesis addresses this conjecture to some extent, as activated EBV-specific T-cells will traffic to the CNS and inhibit the impact of EBV infection.
Further reading
Paper of interest
Background and purpose: Elderly people with multiple sclerosis (pwMS) present higher probability of malignancies. Immune checkpoint inhibitors (ICIs) improve cancer prognosis but pose risk of disease flares in people with pre-existing autoimmune conditions, including MS. Data addressing the impact of ICIs on MS are scarce. This systematic review and meta-analysis evaluates the effects of ICIs on MS disease activity.
Methods: A systematic literature search in Google Scholar and PubMed, following PRISMA 2020 guidelines, identified five observational studies. Data on clinical and neuroradiological outcomes were analyzed using random-effects models.
Results: The clinical activity meta-analysis included 90 pwMS undergoing ICI therapy (median follow-up = 0.62-1.85 years, 103.74 patient-years). The pooled relapse rate was 5.45 per 100 patient-years (95% confidence interval [CI] = 1.86-14.92). Median time to relapse was 1 month after the ICI start (range = 0.4-6 months). No relapse occurred after 58 years. The neuroradiological activity meta-analysis was conducted on 36 pwMS (median magnetic resonance imaging [MRI] follow-up = 0.75-1.85 years, 41.94 patient-years). The pooled new MRI lesion rate was 24.9 per 100 patient-years (95% CI = 10.9-47.3), with median time to new MRI lesions of 3 months (range = 1-6 months). In 80% of cases, disease-modifying treatment (DMT) was suspended at ICI initiation.
Conclusions: We found a low relapse rate in pwMS following ICI treatment, with no events in older pwMS. The risk of neuroradiological activity appears higher, but mainly occurs in pwMS who discontinued DMT. All events occurred within the first 6 months of ICI therapy. These conclusions are based on small observational studies, highlighting the urgent need for further research on this topic.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. You must be a paying subscriber if people want to ask questions unrelated to the Newsletters or Podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
🖋 Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.








Share this post