




Case study
I am 32-years of age and have relapsing-remitting MS. I have been on ocrelizumab for just over 2-years. Since starting ocrelizumab I have had two serious chest infections, which required admission to the hospital. I have also had a serious infusion reaction from which I thankfully recovered. I have also experienced progressive worsening of neurological symptoms with MRI confirmation of relapse on the drug.
Prof G’s opinion
Serious infections
Yes, ocrelizumab is associated with serious infections in a similar way to all immunosuppressive therapies (see Hauser et al. Neurology. 2021 Oct 19;97(16):e1546-e1559).
“In 5,680 in pwMS who received ocrelizumab (18,218 patient-years of exposure) in clinical trials rates per 100 patient-years of serious adverse events was 7.3, infusion-related reactions 25.9, infections 76.2, serious infections 2.01 and malignancies 0.46.”
In other words for every 1,000 pwMS treated for 12 months, 2 pwMS had a serious infection typically requiring hospitalisation. The corollary is that 998 out of 1,000 pwMS treated with ocrelizumab for a year will not have serious infections. So as someone with two serious infections after starting ocrelizumab you are extremely unlucky or you have a risk factor that increases your chances of serious infections. I would recommend you see an immunologist to rule out another confounding factor.
Please note that these serious infections on anti-CD20 therapies tend to occur in older patients (>50 years of age), who are more disabled (EDSS>=6.0), have multiple comorbidities and have hypogammaglobulinaemia. Some of these serious infections with encapsulated bacteria, such as pneumococcus, meningococcus and Haemophilus influenzae, can be derisked by having vaccines prior to starting treatment. In adults in the UK, we only recommend pneumococcal vaccination as a routine. Meningococcus and H. influenzae vaccines are only recommended for pwMS, who are at higher risk of being exposed to these infections, such as students and military recruits.
In pwMS on an anti-CD20 therapy who develop hypogammaglobulinaemia, there is no consensus on immunoglobulin (Ig) replacement therapy. However, in paediatric and some adults patients with non-MS autoimmune diseases on anti-CD20 therapies, Ig replacement therapy tends to be given if patients have a history of recurrent infections. These diseases are not necessarily analogous to MS as most of these diseases are rare with few other treatment options available to these patients. At present Ig replacement therapy to reduce infectious complications as a consequence of anti-CD20 therapies, such as ocrelizumab, is not covered routinely by the NHS.
Another option for recurrent infections is antibiotic prophylaxis. The latter is what is done in patients who have had a splenectomy. Typically this is standard penicillin prophylaxis to cover pneumococcal and meningococcal infection.
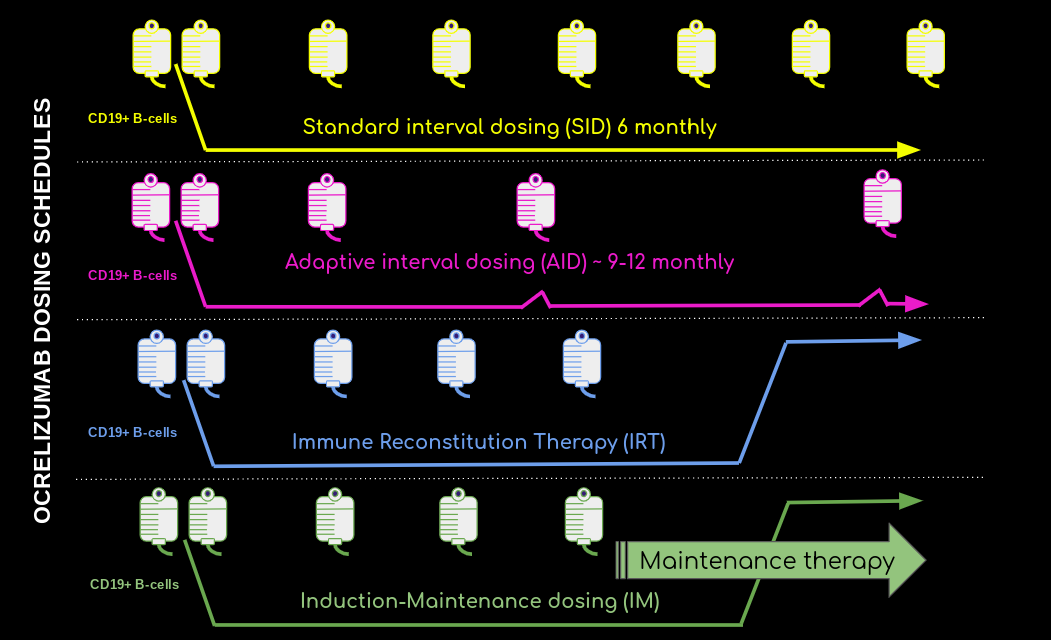
Adaptive dosing
I am aware that a lot of my colleagues, in the UK and internationally, are promoting adaptive dosing of ocrelizumab, based on B-cell reconstitution, to reduce the risk of infection. They are basing their strategy on the ocrelizumab phase 2 extension study when study subjects had 3 or 4 courses of ocrelizumab followed by a non-treatment period of 18 months (Baker et al. Mult Scler Relat Disord. 2020 Sep;44:102279). Yes, the infection risk dropped once the B-cell population is reconstituted. However, an 18-month wash-out is really an immune reconstitution therapy (IRT) strategy with the majority of subjects being allowed to recover their B-cell counts to above the lower limit of normal. This is not the equivalent of the most commonly used adaptive dosing strategy, which is to redose ocrelizumab once the peripheral B-cell counts recover to above 0.5% of the total lymphocyte count, which is at a B-cell count way below the lower limit of normal and occurs at approximately 9 months after the last ocrelizumab infusion. To date, I am not aware of this type of ocrelizumab dosing being safer than continuous 6-monthly dosing (see Sahi et al. Mult Scler Relat Disord. 2021 Nov;56:103287 and Rolfes et al. Neurol Neuroimmunol Neuroinflamm. 2021 Jul 14;8(5):e1035). Please note that these two studies are small, non-controlled, and are simply not of good enough quality to change clinical practice in relation to relative efficacy and safety of anti-CD20 standard interval dosing (SID) vs. adapted internal dosing (AID).
It is clear the MS community are extrapolating data from the Swedish rituximab MS cohort (Salzer et al. Neurology. 2016 Nov 15;87(20):2074-2081.). Although there is no uniform dosing of rituximab in Sweden they stratified their cohort into lower (< 750mg/year) and higher (> 750 mg/year) exposure groups. The MRI and relapse activity appeared equal between these groups and so did safety with very similar immunoglobulin trajectories. This is why I think it premature to assume the AID of ocrelizumab, as currently being used, is going to be safer than SID ocrelizumab and is the main reason why we need to do an appropriately powered trial (ADIOS Study) to test the hypothesis before adopting AID into clinical practice as being the safer option. Please note I have made the point that when it comes to inflammatory MS disease activity, i.e. relapses and MRI activity there is a floor effect, but not necessarily in relation to disability progression or smouldering MS (see Newsletter 2nd-Jan-2022). This is why we can’t accept that these two dosing levels of rituximab are equally efficacious based on NEIDA (no evident inflammatory disease activity) either and is another reason for doing the ADIOS trial.
COVID-19 vaccines
I am aware that we have been giving our patients a choice whether or not to continue with 6-monthly ocrelizumab infusions or to delay dosing for 3-6 months to allow some B-cell reconstitution so that they can make an antibody response to the COVID-19 vaccines. Based on early rituximab data I even recommended a level of 10 B-cells per millilitre of blood as predicting an antibody response to the COVID-19 vaccines. The fact is that in most of these B-cell reconstituted patients who make an antibody response the titres or levels of antibody tend to be low, i.e. at a level that is probably too low to protect them from being infected with the Omicron variant, which escapes immunity at low antibody levels. Fortunately, the latter is not that important in that (1) we now have effective coronavirus antivirals to cover vulnerable patients who get COVID-19, (2) the Omicron variant is less severe, (3) vaccinated anti-CD20 treated patients have T-cell immunity that should protect them from getting severe COVID-19 and (4) we have other treatments to reduce the severity of COVID-19.
I remain to be convinced that ocrelizumab AID to ensure vaccine responses is in fact improving outcomes. What we are lacking is both the adverse event and clinical outcome data on COVID-19 and other infections in patients with MS on continuous 6-monthly SID compared to those on delayed AID.
Please be aware that using AID, in the way it is being implemented at present, to improve safety is unproven in relation to ocrelizumab and comes with the possibility of blunted effectiveness, particularly in relation to disability progression and smouldering MS. I discussed this issue in detail in my previous Newsletter on whether or not we are ready for AID of ocrelizumab (2nd-Jan-2022).
It is also clear that COVID-19 will almost certainly become endemic with the potential of new/seasonal vaccines to cover new strains as they emerge. In addition, there is seasonal flu and countless other emerging viral infections, e.g. Zika virus, and existing exotic viral infections, e.g. dengue and yellow fever. How are we going to be dealing with these infections and the vaccine landscape going forward in anti-CD20 treated patients? My answer is MS is a really bad disease and anti-CD20 and other immunosuppressive therapies have changed the prognosis of this disease to such an extent that it is hard to recognise the same disease in 2022 compared to what we used to see in the pre-DMT era. The majority of pwMS don’t really have alternatives to immunosuppression to treat their MS so you are going to have to accept the risks, live with them, but remain vigilant and be proactive with any infections you may develop.
I also want to stress that the risk of serious infection is really quite low with MS DMTs (see above). The fact that this patient has had two serious infections early in her treatment history is very unusual. This may suggest she has an underlying predisposition to infections. The latter was seen in the phase 3 rheumatoid arthritis ocrelizumab programme, particularly in patients with Asian ancestry (Emery et al. PLoS One. 2014 Feb 3;9(2):e87379). To the best of my knowledge, I am not aware of pwMS with African or Asian ancestry on ocrelizumab being at greater risk of serious infections. However, I stand to be corrected on this.
Infusion reactions and breakthrough disease activity
As you know infusion reactions occur most commonly with the first half-dose infusion and drop off with time. The fact that you had a severe and delayed infusion reaction suggests you may have anti-drug antibodies (ADAs), which not only cause allergic-type reactions but can also be neutralising and stop ocrelizumab from depleting B-cells. Patients with ADAs are more likely to have breakthrough disease activity. It is easy to find out if you have neutralising ADAs. All you need to do is to ask your neurologist to check your peripheral B-cell counts. If you are not B-cell depleted the odds are you have neutralizing antibodies or ADAs and you should stop ocrelizumab and start another DMT.
Conclusion
The apparent ‘evidence of absence’ i.e. no difference in efficacy and/or safety between SID and AID of ocrelizumab and other anti-CD20 therapies, should not be accepted in the ‘absence of evidence’ i.e. no controlled trials.
Subscriptions/Donations
Access to MS-Selfie and the microsite, which is currently been worked on by a medical writer and web designer, will be free to all readers. Paying subscribers and future paying subscribers are kindly supporting the site for everyone. Thank you.
If you have found this Newsletter helpful and/or of interest please feel free to forward it to other people who may find this information helpful.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust. The advice is intended as general advice and should not be interpreted as being personal clinical advice. If you have problems please tell your own healthcare professional who will be able to help you.









Share this post