


Because I refer to smouldering MS as the ‘real MS, and play down the importance of relapses and focal MRI activity in driving MS disability, I am increasingly being asked if everyone with MS has smouldering MS. The answer is NO. And does everyone with smouldering MS end up in a wheelchair? Again the answer is NO. Once you have been identified with smouldering MS do you get relentlessly worse. NO.
No, no and no needs repeating.

I was asked some of these questions by one of my patients in clinic yesterday. He has been successfully treated with alemtuzumab in 2018 and 2019. Despite having no relapses and no new MS disease activity on MRI, he is aware of worsening lower limb function and is having increasing problems with his bladder, bowel and sexual function. Over the last two years, his mobility has decreased to about 10 minutes or 400-500m walking time. Whenever he walks, his right leg begins to drag, and he develops a drop in his right foot. The latter has resulted in him stumbling and having several falls. Last year, he fractured a metatarsal or foot bone as a result of a fall.
This patient missed out on being treated early with alemtuzumab and was only treated several years after diagnosis. He had a delayed diagnosis and spent several years on glatiramer acetate before being able to access alemtuzumab.
His consultation was longer than usual. The outcome of the consultation will lead to several interventions:
He needs an appointment in the walking clinic for a trial of fampridine and possibly a functional electrical nerve stimulator (FES). If he can't tolerate a FES, he will need a bespoke ankle foot orthosis (AFO). In the interim, I recommended that he purchase and use a foot-up device.

Self-help foot-up device I triggered a community physiotherapy assessment for rehabilitation or exercise programmes for his lower limb function. He needs to start using a walking stick to help him prevent any further falls.
He has to have a DEXA or bone density scan to see if he is osteopaenic or osteoporotic. The orthopaedic surgeon managing his metatarsal fracture did not consider MS-related osteoporosis. I suspect this oversight was because he is relatively young, and osteoporosis is uncommon in men.
I referred him to the continence service for a postmicturition volume assessment. This will tell us if he needs to start intermittent self-catheterisation (ISC) to deal with urinary urgency and hesitancy. I started a trial of Mirabegron for his urinary frequency and nocturia. The recommended starting dose was 25mg, which could be increased to 50mg if there was a poor response to the 25mg dose. I also gave instructions to his family doctor about a trial of DDAVP (Desmotabs or Desmospray) for his nocturia. For his hesitancy I suggest trying a lower abdominal vibrator and running water. These can sometimes lead to relaxation of the bladder sphincter.
I spent a lot of time advising on his MS-related constipation and bowel urgency. We are going to start with atrial of senna, 1-2 tablets at night, in combination of lactulose (15-30mL) and a glycerine suppository each morning to have a bowel action. If the glycerine suppository should fail, he will try Microlax mini-enemas and as a back-up we have the option of using anorectal irrigation (e.g. Peristeen system). This patient had had a few episodes of faecal urge incontinence and wants to avoid this happening in the future, hence the proactive approach to managing his bowel function.
The next issue was sexual dysfunction. As a start, he will have a trial of tadalafil (Cialis), and if this fails, to add on top of the tadalafil a small dose of sildenafil (Viagra). Yes, the combination of these two drugs works better than either drug alone. Failing this he will need to go to the sexual dysfunction clinic.
Another issue was his poor sleep. He complained of interrupted sleep and not feeling refreshed on awakening in the morning. I suspect his sleep problem is due to his bladder dysfunction and will improve on Mirabegron and/or DDAVP. However, as he is a heavy snorer, I have asked for him to have a sleep study to exclude obstructive sleep apnoea (OSA). As you are aware, OSA is common in pwMS.

He wanted to know why he was getting worse and whether or not I could predict if and when he would need a wheelchair. He wanted to know if there were any other treatments I could give him to slow down his worsening lower limb function. These question triggered my usual explanation about why pwMS worsen despite being NEIDA (no evident inflammatory disease activity). I referred him to the MS-Selfie Newsletter ‘Getting Worse’ (02-Jul-2021) and have also referred him for screening for the SIZOMUS trial, an add-on study to assess the safety and efficacy of Ixazomib in patients with MS. This treatment aims to target CNS resident plasma and B-cells one of the many drivers of smouldering MS.
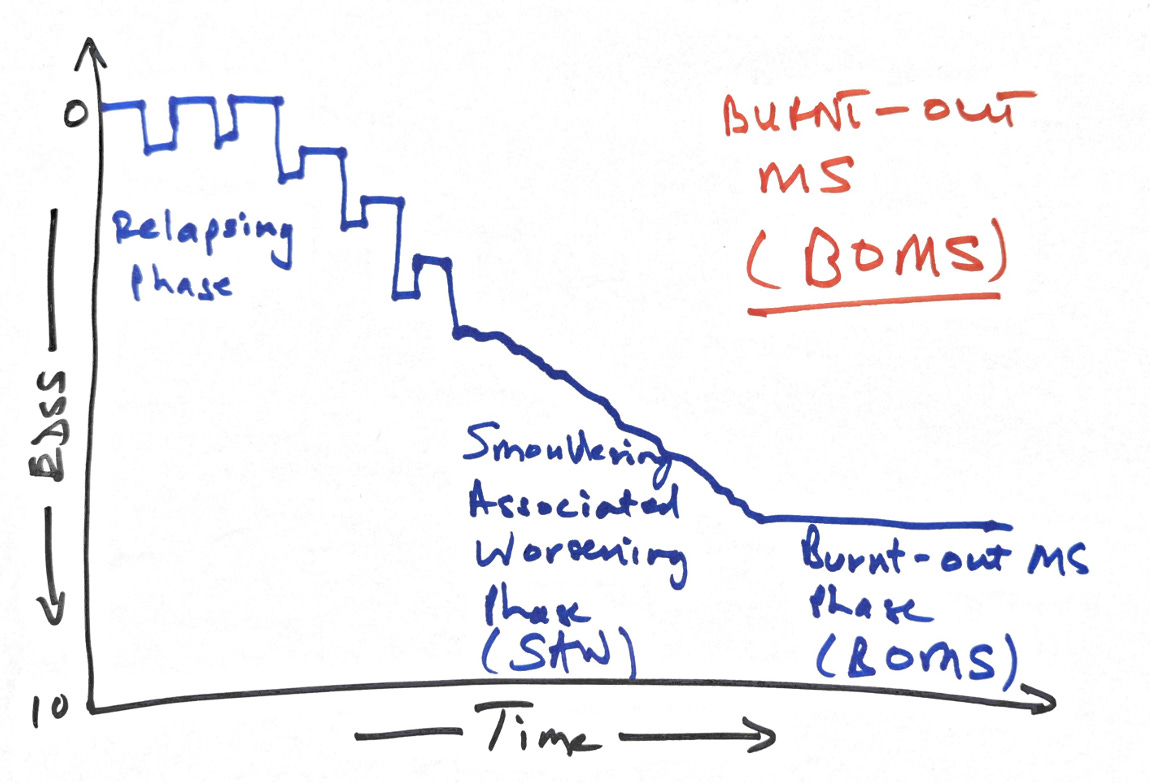
I also mentioned to him the concept of burnt-out MS, i.e. that worsening MS continues for a time until all the nerve fibres destined to degenerate from previous damage die off, leaving behind a pool of surviving nerve fibres that maintain function at a similar level for decades until ageing mechanisms start to impact function later in life.
Professor WI (Ian) McDonald, one of my clinical mentors when I started in the field of MS, pointed out that in his experience, a minority of patients with worsening MS would continue to worsen for several years. Then, they would stop getting worse as if their disease burnt itself out. He used to tell his patients this in his clinic, claiming that about 1 in 10 patients or 10%, would develop this. He referred to this as a burnt-out MS (BOMS).
Burnt-out MS is a controversial topic not covered in the literature. Many commentators mix up the concept of BOMS with benign MS. By definition, ‘benign MS’ is having MS for an extended period with little or no disability. In comparison, BOMS is flat-lining regarding disability worsening after a period of smouldering-associated worsening (SAW).
As I enter the twilight of my career, I agree with Prof. McDonald’s observation with the one proviso that many patients with BOMS, who may be stable for decades, often come back when they get older, with deterioration in function likely to be age-related.
The flatlining after a period of SAW represents therapeutic lag, i.e., it takes time for the anti-inflammatory effect of treatment to manifest, just as it takes time for the damage from past activity to manifest itself fully. In addition, some of the pathologies that underpin smouldering MS may also burn out with time. For example, paramagnetic iron-rimmed lesions on MRI (PRLs), which are thought to expand slowly over time, may stop expanding after several years.
I then had to break the news to this patient that I was partially retiring and that he would have to be seen by one of my colleagues in the future. This generated a lot of discussion about my career plans going forward. If my retirement is news to you please read my recent newsletter ‘Prof G is retiring’ (21-Jun-2024).
Several other problems this patient had that we could not sort out during this visit were chronic lower back pain, which is common in people with more advanced MS, nocturnal limb jerks, low mood and anxiety. In addition, his autoimmune thyroid disease post-alemtuzumab was not being well managed. His last thyroid function tests showed he was still hyperthyroid. Instead of managing this myself, I asked him to contact the endocrine team. He also had on his list of questions for me regarding supplements (which ones to take), exercise (how to do HIIT with weak legs), AHSCT (should he go abroad for AHSCT) and news about remyelination trials. I didn’t have time to answer these questions and referred him to MS-Selfie for answers.
Other aspect of marginal gains approach to the management of MS I could not address included metabolic and social health, diet and alcohol consumption, comorbidities and a detailed review of his current medications. For example, he takes regular antihistamines for hay fever and I want to discuss with him the impact these could be having on his brain health. Sadly, I didn’t have time for this.
The NHS expects us to do MS follow-up consultations in 10-15 minutes. This consultation took over 35 minutes and could have lasted an hour. Thankfully, he had done his self-monitoring (web-EDSS, T25FW, 9HPT and online SDMT), so I did not have to do a neurological examination and formal EDSS. We didn’t even have time to discuss his self-monitoring results.
This patient expected more from his follow-up consultation than I could offer him. What is the solution? What would you recommend to address the problem of needing more time for follow-up consultations?
If he had been an MS-Selfie subscriber and read all the self-help newsletters, he could have sorted out many of his problems. Is this a realistic expectation? Or do people with more advanced MS need an annual MOT? Is MS self-management a pipedream?
For non-British people, an MOT refers to the annual requirement of the UK’s Ministry of Transport (MOT) for motor vehicles to have a service and certificate of roadworthiness before being driven on public roads. In an MOT, the motor vehicle is checked and has preventative maintenance done to prevent breakdowns in the future and, importantly, to ensure the car is safe to drive. All I can say is this person with MS had an incomplete and rather shoddy MOT.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. You must be a paying subscriber if people want to ask questions unrelated to the Newsletters or Podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
X (Twitter) / LinkedIn / Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.








