


The reason why rheumatologists are ahead of us in treating rheumatoid arthritis (RA) and protecting joints (the RA end-organ) is that they have an inflammatory biomarker that is closely linked to outcome, it is called the C-reactive protein (CRP), which they include as part of their treatment target. They also include a PROM (patient-related outcome measure) as part of the DAS (disease activity score); this not only involves RA patients in their treatment but gives patients with RA a deeper understanding of what DMARDs (Disease-Modifying Anti-Rheumatic Drugs) are and what they do to their disease.
If you have RA you want the area under the CRP curve to be as flat as possible to give you the maximum chance of having healthy joints when you get older.
In MS we need both a CRP and a PROM to be part of our treatment target. Do you agree?

Peripheral blood neurofilament levels
The CRP allows rheumatologists to rapidly assess if inflammation is under control. The area under the CRP curve correlates with joint damage in the future, therefore, rheumatologists like to flatten the CRP curve. The good news is that we now have the equivalent of the CRP in the form of plasma neurofilament light chain (NFL) levels. Importantly, the FDA has just granted the Simoa plasma NFL assay Breakthrough Device designation as a prognostic aid in assessing the risk of disease activity in patients diagnosed with relapsing-remitting MS (RRMS). This FDA program is designed to enable rapid development, assessment and review, with the intention to provide pwMS with more timely access to breakthrough technologies or devices. Please note this FDA’s Breakthrough Device designation does not guarantee the NFL assay will be approved.
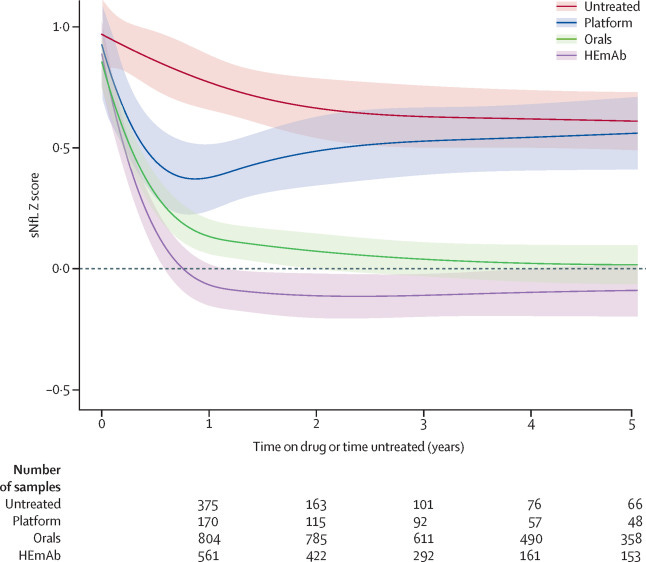
It is clear that NFL is a biomarker of neuroaxonal damage in patients with active MS. Therefore it is only a matter of time before HCPs and pwMS will want to flatten NFL curves; i.e. peripheral blood NFL levels (pbNFL) will be part of our treatment target. I have little doubt that MS centres with the best average NFL levels in their patients will have the best outcomes. As you can see from the figure below it is clear that pwMS on the most effective DMTs do best; there is a clear hierarchy when it comes to suppressing pbNFL levels; this data also supports flipping the pyramid and starting on one of the most effective DMTs first-line. Who wouldn’t want their NFL levels to be maximally suppressed?
We know that raised NFL levels are a poor prognostic sign and correlate with future MS disability and brain volume loss (end-organ damage). However, we still have several hurdles to get over before pbNFL enters routine clinical practice, but we are getting there and the FDA Breakthrough Device designation is a major step forward. One issue that has been addressed is setting normal levels. The great tragedy, or not, of life is that life is an age-dependent neurodegenerative disease and hence pbNFL increases with age and measurements are also affected by weight. This has been addressed by the development of age-dependent normative data in the form of a so-called z-score. Z-scores can be calculated using an internet-based app generously supplied by the University of Basel.
Patient-related outcome measures (PROMs)
What about a universal MS PROM? There is a debate going on at the moment about which PROMs to collect in routine clinical practice and which ones are sensitive and reactive enough to include in an MS-DAS score. The problem for the field is when you put all the MS PROM experts in a room each has their own favourite PROM and up until now has been difficult to get a consensus on which is the best and most practical to use in routine clinical practice. Another problem is that most of the most widely used PROMs in MS are not well-liked by patients; patients feel that these PROMs don’t really capture the impact that MS is having on their lives. To address this issue the global Patient Reported Outcome for Multiple Sclerosis (PROMS) Initiative has been launched. This is a multi-stakeholder PROMS Initiative that is been jointly led by the European Charcot Foundation (ECF) and the Multiple Sclerosis International Federation (MSIF), with the Italian Multiple Sclerosis Society (AISM) acting as the lead agency for and on behalf of the global MSIF movement. The initiative has the ambitious mission to get a unified view on PROMs for MS (see paper 2 below).
Although I don’t think the PROM issue will be sorted out anytime soon, progress will be made. Therefore, my money is on pbNFL levels and I have little doubt that you will be asking for and tracking your own NFL levels in the near future. At our centre, we have been using NFL levels to monitor MS for over 5 years and it has transformed our practice in terms of defining what is active MS. There is one caveat and that is progressive or smouldering MS and it looks as if NFL is not a good marker to measure the slow neurodegeneration that takes place as part of the smouldering disease. For more information on this, I suggest you read my earlier Newsletter ‘Serum neurofilament levels - another one bites the dust?’ (9-Feb-2022). In this Newsletter I discuss some of the complex issues that need to be considered when using pbNFL to monitor smouldering disease. I suspect these issues will also be explored by the FDA and maybe the reason why pbNFL does not get approved.
Paper 1
Background: Serum neurofilament light chain (sNfL) is a biomarker of neuronal damage that is used not only to monitor disease activity and response to drugs and to prognosticate disease course in people with multiple sclerosis on the group level. The absence of representative reference values to correct for physiological age-dependent increases in sNfL has limited the diagnostic use of this biomarker at an individual level. We aimed to assess the applicability of sNfL for identification of people at risk for future disease activity by establishing a reference database to derive reference values corrected for age and body-mass index (BMI). Furthermore, we used the reference database to test the suitability of sNfL as an endpoint for group-level comparison of effectiveness across disease-modifying therapies.
Methods: For derivation of a reference database of sNfL values, a control group was created, comprising participants with no evidence of CNS disease taking part in four cohort studies in Europe and North America. We modelled the distribution of sNfL concentrations in function of physiological age-related increase and BMI-dependent modulation, to derive percentile and Z score values from this reference database, via a generalised additive model for location, scale, and shape. We tested the reference database in participants with multiple sclerosis in the Swiss Multiple Sclerosis Cohort (SMSC). We compared the association of sNfL Z scores with clinical and MRI characteristics recorded longitudinally to ascertain their respective disease prognostic capacity. We validated these findings in an independent sample of individuals with multiple sclerosis who were followed up in the Swedish Multiple Sclerosis registry.
Findings: We obtained 10 133 blood samples from 5390 people (median samples per patient 1 [IQR 1-2] in the control group). In the control group, sNfL concentrations rose exponentially with age and at a steeper increased rate after approximately 50 years of age. We obtained 7769 samples from 1313 people (median samples per person 6·0 [IQR 3·0-8·0]). In people with multiple sclerosis from the SMSC, sNfL percentiles and Z scores indicated a gradually increased risk for future acute (eg, relapse and lesion formation) and chronic (disability worsening) disease activity. A sNfL Z score above 1·5 was associated with an increased risk of future clinical or MRI disease activity in all people with multiple sclerosis (odds ratio 3·15, 95% CI 2·35-4·23; p<0·0001) and in people considered stable with no evidence of disease activity (2·66, 1·08-6·55; p=0·034). Increased Z scores outperformed absolute raw sNfL cutoff values for diagnostic accuracy. At the group level, the longitudinal course of sNfL Z score values in people with multiple sclerosis from the SMSC decreased to those seen in the control group with use of monoclonal antibodies (ie, alemtuzumab, natalizumab, ocrelizumab, and rituximab) and, to a lesser extent, oral therapies (ie, dimethyl fumarate, fingolimod, siponimod, and teriflunomide). However, longitudinal sNfL Z scores remained elevated with platform compounds (interferons and glatiramer acetate; p<0·0001 for the interaction term between treatment category and treatment duration). Results were fully supported in the validation cohort (n=4341) from the Swedish Multiple Sclerosis registry.
Interpretation: The use of sNfL percentiles and Z scores allows for identification of individual people with multiple sclerosis at risk for a detrimental disease course and suboptimal therapy response beyond clinical and MRI measures, specifically in people with disease activity-free status. Additionally, sNfL might be used as an endpoint for comparing effectiveness across drug classes in pragmatic trials.
Paper 2
On 12 September 2019, the global Patient Reported Outcome for Multiple Sclerosis (PROMS) Initiative was launched at the 35th Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS). The multi-stakeholder PROMS Initiative is jointly led by the European Charcot Foundation (ECF) and the Multiple Sclerosis International Federation (MSIF), with the Italian Multiple Sclerosis Society (AISM) acting as the lead agency for and on behalf of the global MSIF movement. The initiative has the ambitious mission to (i) maximize the impact of science with and of patient input on the life of people affected by MS, and (ii) to represent a unified view on Patient-Reported Outcomes for MS to people affected by MS, healthcare providers, regulatory agencies and Health Technologies Assessments agencies. Equipped with an innovative participatory governance of an international and interdisciplinary network of different stakeholders, PROMS has the potential to guide future breakthroughs in MS patient-focused research and care. In this paper we present the progresses of the global PROMS Initiative and discuss the open questions that we aim to address.
Subscriptions and donations
I am using the paid subscriptions to administer the MS-Selfie Newsletter and associated MS-Selfie microsite that is currently in development. If you are an active paying subscriber thank you, your contribution is much appreciated. At the request of several readers, I have now added the option of making a one-off donation as well. Funds from subscriptions and donations are being used to pay a professional medical writer to curate, rewrite and transfer the contents of the Newsletter onto a companion MS-Selfie microsite, which is being designed and maintained by a freelance web designer.
Thank you.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry or Barts Health NHS Trust. The advice is intended as general advice and should not be interpreted as personal clinical advice. If you have problems please tell your own healthcare professional who will be able to help you.







