




It has been 30 years since I arrived in London from South Africa to do a PhD on the immunology of MS. My research was on soluble biomarkers of inflammation in spinal fluid, blood and urine. I ended up doing my PhD on a single inflammatory biomarker called neopterin. Many of the ideas and hypotheses I formulated in the neuroimmunology laboratory between 1993 and 1996 are still as relevant today as they were 30 years ago.
One of the central hypotheses I promoted, and still do, is that the oligoclonal immunoglobulin response or OCBs (oligoclonal bands) in the cerebrospinal fluid (CSF) of people with MS (pwMS) has to be central to finding out the cause of MS. And that the OCB response is abnormal and is driving MS disease pathology, particularly smouldering MS (slowly expanding, paramagnetic rim, acute demyelinating and the subpial cortical lesions).
The initial driver of the OCB hypothesis was a small study by two of my mentors Prof. Ed Thompson and Prof. Peter Rudge, who showed that cyclosporin-A reduced the number of immunoglobulin-free light chains in the spinal fluid of subjects with MS in a clinical trial (see paper one below).
Cyclosporin A was a revolutionary immunosuppressive therapy that changed the solid organ transplantation landscape (see paper two below) and was tried in chronic progressive MS. Remarkably, cyclosporine was shown to work and slow down MS disease worsening. However, as it was associated with renal toxicity, it was never licensed to treat MS. People seem surprised when I remind them that we had MS disease-modifying therapies in the 1980s, which predate the interferon-beta era. The transplant physicians eventually derisked the renal toxicity associated with cyclosporine, which is why I am surprised it was not taken forward in MS.
Immunoglobulins
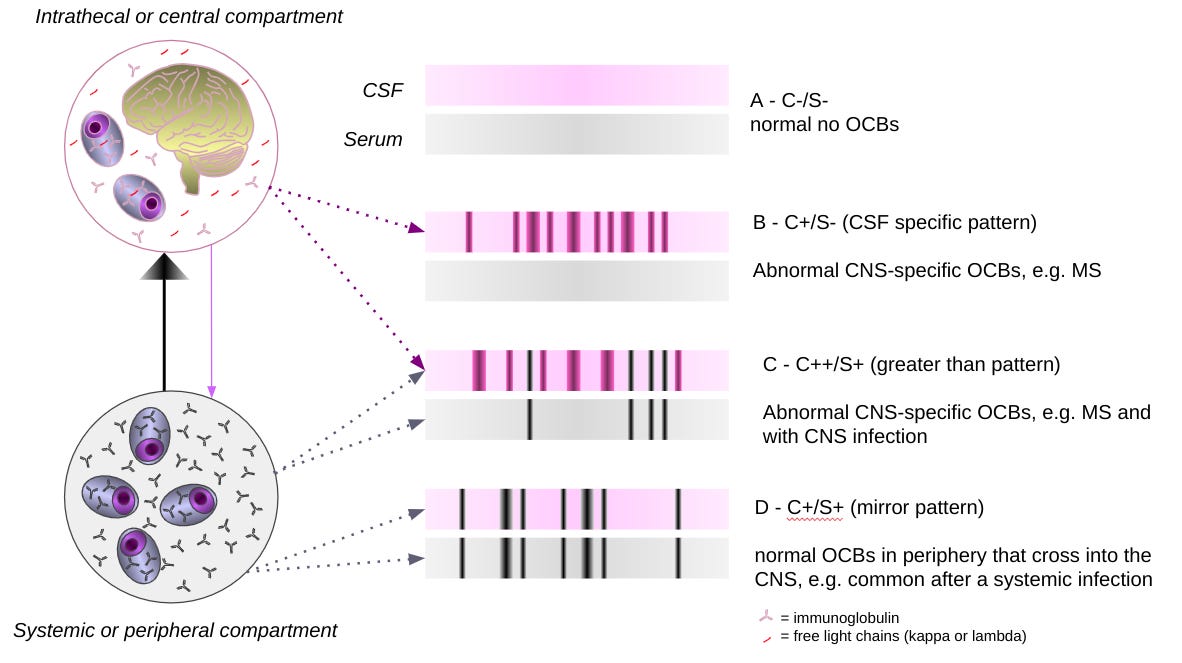
Immunoglobulins (Ig) are formed from two heavy and light chains. The heavy chains are D, M, A, E or G, and IgG is subdivided into IgG1, 2, 3 or 4. There are two Ig light chain classes, kappa and lambda. The B-cells and plasma cells that make Ig make many more light chains than heavy chains. The excess light chains are released into the tissue fluid and CSF. By measuring the amount of Ig free light chains in the spinal fluid, you can determine how active B-cells and plasma cells are in the central nervous system (CNS) of patients with MS, i.e. CSF kappa and lambda light chain levels are an index of B-cell and plasma cell activity in the CNS.

The original observation that cyclosporin reduces CSF Ig light chain levels is a proof-of-concept study; it is evident that if you want to target CNS B-cells and plasma cells, we have the biomarker to show our treatments are working on the target. This is why the latest research findings from Sweden (paper three below), which show that spinal fluid Ig light chain levels correlate with smouldering MS or PIRA (progression independent of relapse activity), are so important. The implication is that if we can scrub the brain clean of B-cells and plasma cells and reduce CNS Ig production, we may slow down or stop smouldering MS. This is why our group is studying the effects of cladribine and ixazomib on CSF Ig free light chains.
We are currently running Cladriplas (subcutaneous cladribine), Clad-B (oral cladribine) and SIZOMUS (ixazomib) trials, which are looking at whether or not these treatments can reduce CSF Ig free light chain kappa and lambda levels. These studies are super exciting and potentially game-changers for the field of MS as we strive to go beyond NEIDA (no evident inflammatory disease activity) and tackle the processes driving smouldering MS.
Other potential therapies targeting CNS B-cells and plasma cells include the CNS-penetrating BTK inhibitors (BTKi) and CD19-targeted CAR T-cells (please see MS-Selfie Newsletter “CAR T-cells as a treatment for MS”, 17-Sept-2022) The BTKIs are close to the market. I would love to know what they do to CSF kappa and lambda Ig light chain levels. I suspect they will reduce CSF Ig light chain levels but are unlikely to scrub the CSF clean of OCBs. Long-lived plasma cells do not require BTK signalling to be kept alive and hence may survive BTK inhibition.
I am also in active discussions around doing an exploratory safety study of anti-CD19 targeted CAR T-cells in MS. The proposal I have put forward includes doing lumbar punctures in patients to look at the impact of this class of treatment on CSF Ig light chain levels. The good thing about CAR T-cells is they travel into the CNS and would clear the CSF of B-cells. Again will this be sufficient, or do we also need CAR T-cells to clear the long-lived plasma cells?
It is nearly 30 years since I developed my first quantitative assays to measure kappa and lambda light chains in both the spinal fluid and urine of pwMS. To see the science evolve to the point where we use these biomarkers as outcome measures in clinical trials is very rewarding. Maybe I didn’t waste time working on kappa and lambda-free light chains in MS?
Paper 1 - Cyclosporine CSF Ig light chain study
Free light chains in the cerebrospinal fluid of patients with multiple sclerosis correlate closely with disease activity. As part of a double-blind placebo-controlled trial of immunosuppression using cyclosporin A in patients with multiple sclerosis, light chain analysis was performed on pre- and post-treatment CSF samples in 19 patients, nine having received cyclosporin A and 10 placebo. The placebo-treated patients showed continued immunological activity, as evidenced by an increase in both free kappa and lambda chains, but cyclosporin A treatment resulted in no change or an improvement in light chain response, indicative of suppression of continued activity. As cyclosporin A does not enter the CSF, this implies that systemic stimulation is at least partly responsible for continued disease activity in multiple sclerosis. Cyclosporin A may thus be effective in preventing the deterioration of patients with multiple sclerosis.
Paper 2 - Cyclosporine trial
Patients with clinically definite multiple sclerosis, mild to moderately severe neurological disability (entry score on the Expanded Disability Status Scale (EDSS) between 3.0 and 7.0), and a progressive course defined by an increase in the EDSS of between 1 and 3 grades in the year prior to entry were randomized to receive either cyclosporine (n = 273) or placebo (n = 274) in a 2-year, double-blinded, multicenter trial. Treatment groups at entry proved balanced for age, gender, duration of illness, and neurological disability. Cyclosporine dosage was adjusted for toxicity and a median trough whole-blood level was maintained between 310 and 430 ng/ml. The mean increase in EDSS score was 0.39 +/- 1.07 grades for cyclosporine-treated patients and 0.65 +/- 1.08 grades for placebo-treated patients from entry until the time of early withdrawal or completion of the study (p = 0.002). Of three primary efficacy criteria, cyclosporine delayed the time to becoming wheelchair bound (p = 0.038; relative risk, 0.765), but statistically significant effects were not observed for "time to sustained progression" or on a composite score of "activities of daily living." Active treatment did have a favorable effect on several secondary measures of disease outcome. A large and differential withdrawal rate (44% for cyclosporine-treated patients, 32% for placebo-treated patients) complicated the analysis but did not appear to explain the observed effect of cyclosporine in delaying disease progression. Multivariate analysis did not show institutional effects but did demonstrate substantial effects of baseline neurological disability on outcome. Nephrotoxicity and hypertension were common troublesome toxicities and accounted for most of the excess loss of patients in the cyclosporine arm of the study. Thus, chronic cyclosporine therapy was associated with a statistically significant but clinically modest delay of progression of disability in a group of patients with multiple sclerosis selected for moderately severe and progressive disease. Close supervision by physicians familiar with cyclosporine is mandatory to minimize known adverse effects, particularly nephrotoxicity, when considering the use of this immunosuppressant.
Paper 3 - Swedish CSF light chain PIRA study
Background: While kappa free light chain (KFLC) index has become a useful diagnostic biomarker in multiple sclerosis (MS), its prognostic properties are less explored. B cells play a crucial role in MS pathogenesis, but the impact from increased intrathecal production of immunoglobulins and KFLC remains to be determined. Recently, it has become evident that insidious worsening is not confined to progressive MS but is also common in relapsing-remitting MS (RRMS), a feature known as progression independent of relapse activity (PIRA).
Methods: We retrospectively identified 131 patients with clinically isolated syndrome or early RRMS who had determined KFLC index as part of their diagnostic workup. Demographic and clinical data were extracted from the Swedish MS registry. Associations of baseline KFLC index with evidence of disease activity (EDA) and PIRA were investigated in multivariable cox proportional hazards regression models.
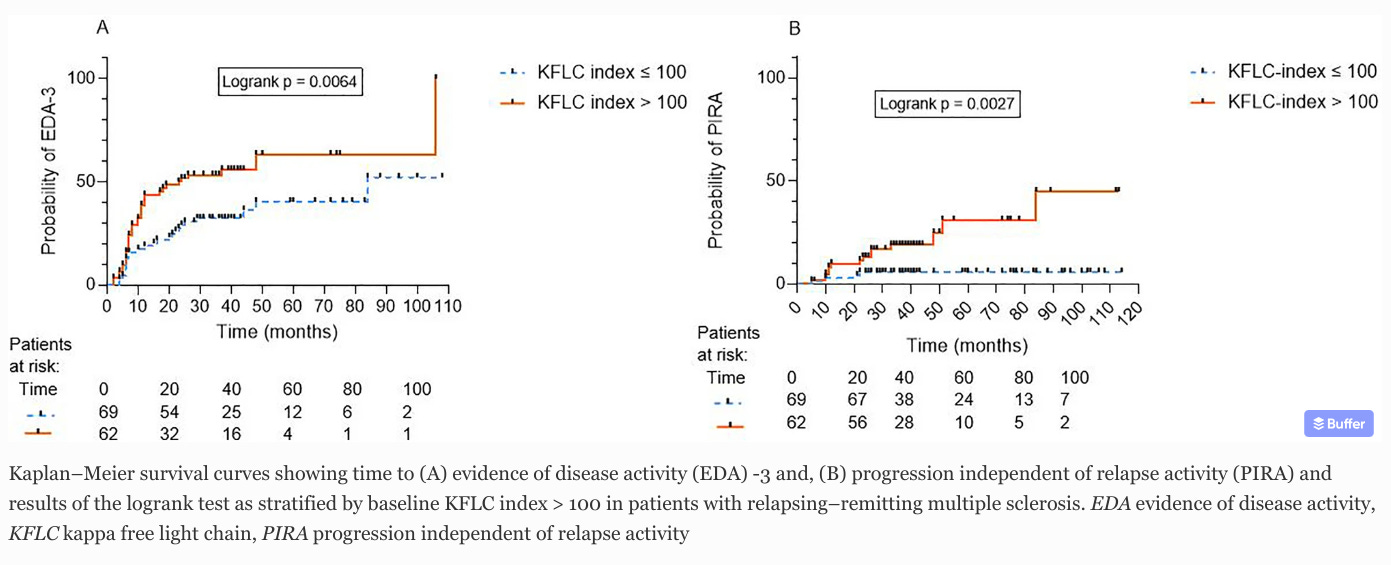
Results: KFLC index was significantly higher in PIRA (median 148.5, interquartile range [IQR] 106.9-253.5) compared with non-PIRA (78.26, IQR 28.93-186.5, p = 0.009). In a multivariable cox regression model adjusted for confounders, KFLC index emerged as an independent risk factor for PIRA (adjusted hazard ratio [aHR] 1.005, 95% confidence interval [CI] 1.002-1.008, p = 0.002). Dichotomized by the cut-off value KFLC index > 100, patients with KFLC index > 100 had an almost fourfold increase in the risk for developing PIRA. KFLC index was also predictive of evidence of disease activity during follow-up.
Conclusions: Our data indicate that high KFLC index at baseline is predictive of PIRA, EDA-3, and overall worse prognosis in MS.
Paper 4 - Urine FLCs in MS
Background: Plasma and B cells are implicated in multiple sclerosis (MS) and produce free light chains (FLC) that are excreted in urine.
Objective: To confirm that demyelinating diseases (DD) cause increased urinary FLCs.
Method: Urinary FLC in 50 patients with DD were compared to 20 patients with posterior uveitis (PU), 19 with AIDS, 34 with rheumatoid arthritis (RA) and 19 normal controls (NC).
Result: Subjects with DD, PU, RA and AIDS have higher urinary FLCs than NC (p<0.01). Urinary FLCs did not correlate with gadolinium-enhancing lesions on MRI.
Conclusions: Urinary FLCs are raised in DD. Further studies are required to see if they correlate with disease activity.
Subscriptions and donations
Paid subscriptions to MS-Selfie are being used to administer the Newsletter and associated MS-Selfie microsite, which is now open to all readers. At the request of several readers, I have now added the option of making a one-off donation. To keep this initiative open to all readers, I would appreciate it if those who can afford a subscription to subscribe. For active paying subscribers, thank you; your contribution is much appreciated. Because of the falloff in paying subscribers, I am considering returning to a paywall that will give paying subscribers six months of unlimited access to all newsletters. At the same time, free subscribers will have a wait to access the newsletters later, not as an email, but on the substack site.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.







Share this post