



During the development, subsequent licensing and use of therapies for more advanced MS, I repeatedly made the point that the MS community must manage expectations, i.e. what is a realistic expectation for people on these therapies. It is clear we have not done so and that people with MS (pwMS) are disappointed with these therapies' impact on advanced (aka progressive) MS. More and more patients are getting angry with me that they are still getting worse despite being on treatment. Every week I have to deal with disappointment from broken promises based on over-hyped expectations. The following is a survey I did via the MS Blog several years ago, showing how we, the MS community, have created unrealistic expectations.
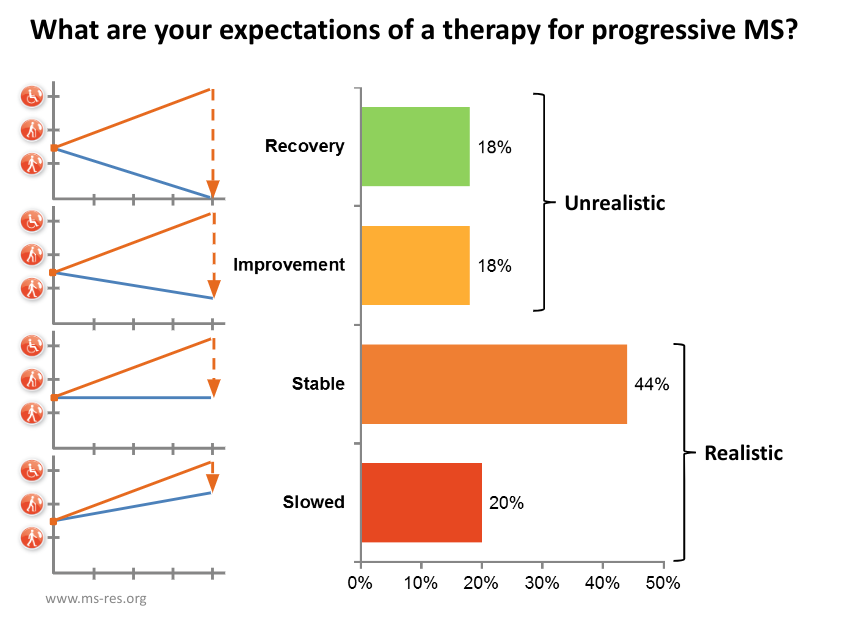
The problem is that licensed treatments for progressive MS, siponimod for SPMS, and ocrelizumab for PPMS don’t stop disability from worsening but only slow down its acquisition. Therefore, pwMS on these treatments think they are not working. It is natural for you to get frustrated and ask for more. Identifying smouldering-associated worsening in people with very early MS, even in people with radiologically-isolated syndromes (RIS) or clinically-isolated syndromes (CIS), has exacerbated this disappointment. I know this is bad news, but it is the reality, and unless we identify and define smouldering MS, we won’t develop the next generation of treatments to tackle this problem. Please don’t shoot the messenger.
I want to remind the MS community that we haven’t cracked MS yet. We may have effective therapies to stop focal inflammatory events (relapses and new MRI lesions). Still, we are far from stopping smouldering MS and the impact of early ageing on the progressive loss of physical and cognitive functioning. I can say that our anti-inflammatory therapies do slow down the rate of worsening, so pwMS should only expect to face disability milestones much further in the future.
The one exception is the impact of immune reconstitution therapies used very early in the course of MS. We are now seeing a minority of pwMS treated early with alemtuzumab or AHSCT and possibly with cladribine in long-term remission with normalised end-organ damage markers, who are functioning normally. In other words, these pwMS don’t seem to have evidence of ongoing smouldering MS. I suspect some of these people may even be cured of having MS.
I have been heavily criticised for daring to mention the C-word. How can you ever be cured of having MS? Despite these observations, I get increasing push-back from colleagues and others in the MS community for wanting to use IRT (immune reconstitution therapies) very early in the course of the disease. Therein lies the problem. Many of these colleagues are satisfied with the treatment target of NEIDA (no evident inflammatory disease activity) without thinking about the end organ, smouldering MS and what causes MS. Herein lies the problem.
I am convinced we already have data to show we can cure a minority of pwMS, but the MS community does not want to look for a cure. If they did, they would be forced to adopt a treatment strategy that could increase the chances of finding an MS cure. I find this very sad. Maybe it is time to hang up my gloves and accept defeat.
Subscriptions and donations
Paid subscriptions to MS-Selfie are being used to administer the Newsletter and associated MS-Selfie microsite, which is now open to all readers. At the request of several readers, I have now added the option of making a one-off donation. To keep this initiative open to all readers, I would appreciate it if those who can afford a subscription to subscribe. For active paying subscribers, thank you; your contribution is much appreciated. Because of the falloff in paying subscribers, I am considering returning to a paywall that will give paying subscribers six months of unlimited access to all newsletters. At the same time, free subscribers will have a wait to access the newsletters later, not as an email, but on the substack site.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your own healthcare professional, who will be able to help you.









Share this post