




Case Study
Hello. I am a 38-year-old woman diagnosed with MS in 2002.
Here is my story:
Optic neuritis right eye 2000.
Diagnosed with MS in 2014 after presenting with left optic neuritis
Relapses followed in 2014 with numbness and heaviness of left leg and in 2015 decreased balance requiring a walking stick to mobilise.
Treated with Alemtuzumab in 2016 and 2017.
Developed hyperthyroidism after alemtuzumab treatment.
Unfortunately, I have developed L’hermitte’s phenomenon and my most recent MRI (October 2021) showed a new spinal cord lesion at C4.
My neurologist has advised a course of steroids, followed by treatment with either Cladribine, Ocrelizumab, Ofatumumab or Natalizumab.
My preference, based on having five “good” years, and my personal situation is to have a third course of Alemtuzumab, but have been refused on the grounds that I have previously been diagnosed with another autoimmune condition, i.e. thyroid autoimmunity.
I really do not know where to go with this. Would you recommend I seek a second opinion from a different neurologist?
The data on the other DMTs is confounding.
Prof G’s Opinion
I completely agree with you and disagree with your neurologist. The European Medicine Agency’s (EMA) decision to make another autoimmune contraindication is a thumb-suck and not based on the evidence.
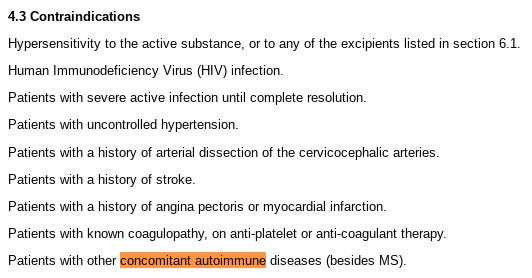
We the MS community with an interest in making alemtuzumab available to as many people with MS as possible tried to convince the EMA that this was not necessary, but they refused to listen to us the MS experts with experience in using alemtuzumab and ignored the data. Please note the following list of contraindications to alemtuzumab that is currently in alemtuzumab’s summary of product characteristics.
Please note we presented very good data to support our position that autoimmunity should not be a contraindication to alemtuzumab or additional courses but the EMA refused to listen to us. The good news is that we have recently been published this data (see below). I, therefore, suggest you take the article below and show it to your neurologist to see if they will change their minds and if not vote with your feet and get a second opinion.
The Data
Coles et al. Autoimmunity and long-term safety and efficacy of alemtuzumab for multiple sclerosis: Benefit/risk following review of trial and post-marketing data. Mult Scler. 2021 Dec 9;13524585211061335.
Does preexisting or treatment-emergent autoimmunity increase the risk of subsequent autoimmune disease in individuals with relapsing-remitting multiple sclerosis (MS) after alemtuzumab? In the extended phase 2/3 trials, 34/96 (35.4%) patients with and 395/1120 (35.3%) without preexisting autoimmunity developed non-MS autoimmunity. Thyroid autoimmunity after alemtuzumab courses 1 or 2 did not increase subsequent non-thyroid autoimmune adverse events. Therefore, autoimmune disease before or after alemtuzumab treatment does not predict autoimmunity after further courses, so should not preclude adequate alemtuzumab dosing to control MS. Finally, post-marketing safety data contribute toward a full record of the alemtuzumab benefit/risk profile for the MS field.
Further reflections
The experience with EMA around this exact issue of autoimmunity before or after alemtuzumab treatment being a contraindication to using alemtuzumab makes me realise that it is not only individuals that have cognitive biases but also institutions.
Your email has made me realise that we, the UK MS community, don’t have to accept the EMA’s position, and could theoretically ask the MHRA to review this issue. One advantage of Brexit is that it potentially allows us to diverge from the ultra-conservative EMA in issues such as this, particularly when their decisions and rulings make no sense and are not evidence-based.
If anyone from Sanofi-Genzyme is reading this Newsletter can you please discuss this option internally? We need the MHRA to revise alemtuzumab’s SmPC and to take out autoimmunity as being a contraindication to treating someone with MS with alemtuzumab. Thank you.
Subscriptions
As you are aware I am raising funds from paid subscriptions to administer the MS-Selfie Newsletter and associated MS-Selfie microsite that is currently in development. So if you are an active paying subscriber thank you, your contribution is much appreciated.
I originally charged a subscription for case studies such as this and made all the other MS-Selfie newsletters free. I subsequently changed the funding model of MS-Selfie and made all content free. However, since doing this I have had a large number of subscribers cancel their subscriptions, which is now threatening the financial viability of MS-Selfie. If this trend continues, which I hope it will not, I will have to reintroduce a two-tiered system with the case studies being restricted to paying subscribers only.
Please note the money raised via subscriptions is being used to pay a professional medical writer to curate, rewrite and transfer the contents of the Newsletter onto a companion MS-Selfie microsite, which is being designed and maintained by a freelance web designer.
So if you find these Newsletters helpful and want the wider MS community to continue to have access to all content I would encourage you to become a paid subscriber. Thank you.

General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust. The advice is intended as general advice and should not be interpreted as being personal clinical advice. If you have problems please tell your own healthcare professional who will be able to help you.









Share this post