


The MS community has painted itself into a corner with how we classify MS. Neurologists in the UK and the United Arab Emirates (UAE) have just published new treatment guidelines based on the old and arguably outdated classification system that MS can be divided into different clinical categories, i.e. clinically-isolated syndrome (CIS), relapsing-remitting (RRMS), secondary progressive (SPMS) and primary progressive (PPMS). Layered on top of this is whether MS is active or inactive and whether the predicted prognosis is good or bad. The UAE guidelines have also included radiologically isolated syndrome (RIS) or asymptomatic MS in their treatment algorithm. I assume the inclusion of RIS into their treatment algorithm is to pre-empt the new MS diagnostic criteria that will be published later this year.
The problem with these classifiers is that they are all flawed and not underpinned by biology.

MS was divided into multiple subtypes by the pharmaceutical industry to allow interferon-beta-1b to be licensed by the FDA as a treatment for RRMS under the Orphan Drug Act in the US. The Orphan Drug Act incentivises drug development in rare and neglected diseases. To be considered an orphan disease, there have to be fewer than 200,000 people with the disease in the USA. MS could only fulfil the 200,000 rule by being divided into three diseases (RRMS, SPMS and PPMS); later, a fourth category, CIS, was added. This is folly as MS is MS, i.e. it is one disease. From a biological perspective, there are no differences in these four categories. For that matter, RIS, a fifth category that is about to be added as a diagnostic category, is also MS. The FDA has tried to row back on this classification system and now licenses MS DMTs under the categories relapsing forms of MS and PPMS. The same cannot be said for the MHRA and EMA in Europe.
Just so you know, the FDA was complicit with the MS three-or-four disease paradigm when they met with Berlex and MS experts in 1989 to classify MS as an orphan disease. Sadly, we are still suffering the consequences of that flawed decision. The next issue of active versus inactive MS is driven by a clinico-radiological worldview of MS. MS is active if there have been relapses or MRI activity (Gd-enhancing lesions or new or enlarging T2 lesions) in the last 12-36 months. Please note the exact period of time for defining what constitutes active MS is debatable; some use 12 months and others 24 and 36 months to define active MS. In the UK, the definition of active SPMS has even been extended to ‘inactive’ MS if someone is on an existing DMT. The assumption is that the current DMT is suppressing relapses and MRI activity but not helping with the so-called SPMS phase of the disease. This fudge allows us to at least switch patients with smouldering MS on existing DMTs to siponimod (Mayzent), which is licensed in Europe for treating active SPMS.
Have you ever tried telling someone with MS who has NEIDA (no evident inflammatory disease activity) who is getting worse because of smouldering disease that they have inactive MS? The standard response is how can I have inactive MS if I am getting worse. This is one of the reasons why I have had to develop a narrative to explain to pwMS why they are getting worse despite having no focal inflammatory disease activity (please see ‘Getting Worse’; 02-Jul-2021).
I have argued before that superimposed focal inflammatory activity (relapses or new lesions on MRI) is likely to be the immune system’s response to what is causing MS and not MS itself. Relapses and focal MRI activity don’t fulfil contemporary criteria for being a surrogate outcome and are poor predictors of MS disease outcomes. Therefore, they can’t be the primary pathology driving MS. I think the real MS is smouldering MS that may or may not trigger a focal inflammatory event. Please note I am not saying relapses and focal MRI activity don’t matter. Focal inflammation contributes to the underlying damage that occurs in MS, but it is not the primary driver of MS. This is why you use focal inflammation as a treatment target in MS and switch or escalate treatment based on relapses and focal MRI activity. However, a large proportion of people who have NEIDA will still get worse from smouldering MS.
Does this mean all pwMS will have smouldering disease?
Clearly not, as many people found to have pathologically-confirmed MS at post-mortem were never diagnosed as having MS in life; either they didn’t have symptoms or their symptoms were mild and/or atypical and didn’t warrant a diagnostic work-up. Similarly, about 10% of siblings of pwMS have lesions on MRI that look suspicious of MS. However, only 2.5% or a quarter of them go on to develop MS. Similarly, a relatively large proportion of people with RIS never have an MS-defining attack. Presumably, these people diagnosed with RIS during life but don’t develop MS represent those people who are found to have incidental MS at post-mortem and didn’t have smouldering MS in life.
Can you prevent or prevent smouldering MS from developing?
It is also notable that a small percentage of people with MS treated early with immune reconstitution therapies, such as alemtuzumab or AHSCT, go into long-term remission and don’t develop smouldering MS. I have argued in the past that I think some of these people may be cured of their MS.
I keep repeating these points because you can have MS and not develop smouldering disease. I suspect what is happening in this situation is that your immune system finds and eliminates the cause of MS, which prevents the subsequent development of smouldering disease. I think that smouldering MS represents active MS, which is why the term inactive MS is a misnomer.

A counterfactual
As a counterfactual, I would prefer people to have MS or not have MS using a biological definition of MS. Then we can add on descriptors such as recent evident focal inflammatory activity (EIDA) or no recent evident focal inflammatory disease activity (NEIDA) and recent evident smouldering worsening (SAW) or no recent evident smouldering worsening (NSAW). This construct will at least frame future MS drug development, focusing on what to do about SAW. Will switching someone who is NEIDA/SAW from a platform therapy to one of the high-efficiency DMT make a difference? I suspect it may, but we don’t yet have the evidence.

We need new treatment strategies, such as combination treatments targeting both EIDA and SAW, to address the unmet need.
There is one caveat to this counterfactual classification system is that some pwMS who have had MS for decades and have lost a lot of brain and neuronal reserve may be present with delay worsening as a result of superimposed ageing. At the moment, we don’t have a reliable way of identifying or diagnosing this ageing-associated worsening, which will likely require a different therapeutic approach.
I would like to know if you understand the semantics and arguments in this newsletter and whether this has relevance to you as someone with MS.
I sincerely hope we will be able to sort out the diagnosis and classification of MS so that we can start trials in people with smouldering MS to tackle the problem of SAW.
Paper 1 - UK
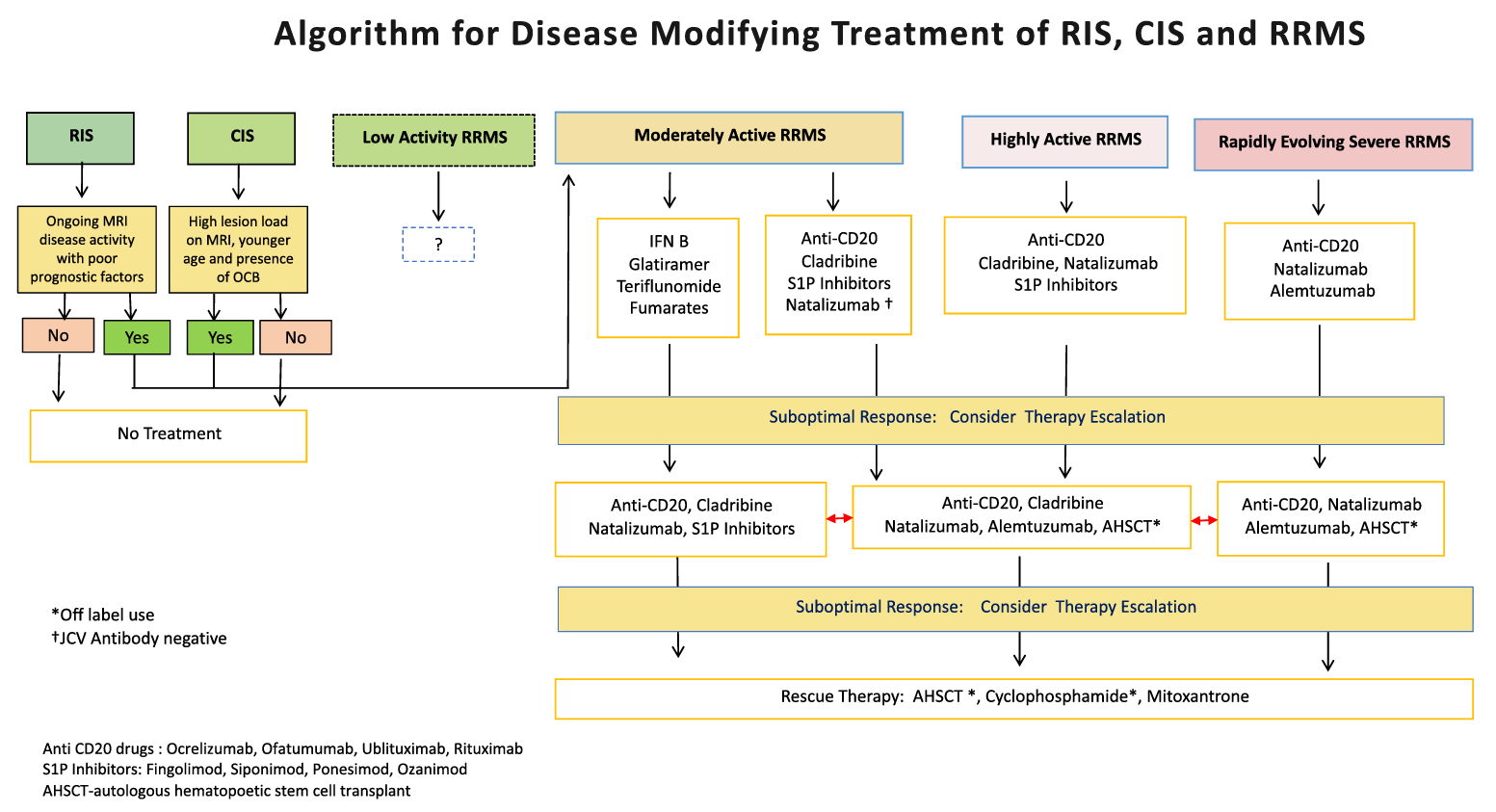
Paper 2 - UAE
The newly constituted National Multiple Sclerosis (MS) Society (NMSS)of the United Arab Emirates (UAE), set up a scientific committee to create a MS disease modifying treatment (DMT) guideline for UAE. The committee considered several unique features of the MS community in UAE including large number of expatriate population, wide variations in health insurance coverage, physician and patient preferences for DMT. The overall goal of the treatment guideline is to facilitate the most appropriate DMT to the widest number of patients. To this end it has adapted recommendations from various health systems and regulatory authorities into a pragmatic amalgamation of best practices from across the world. Importantly where data is unavailable or controversial, a common sense approach is taken rather than leave physicians and patients in limbo. The committee classifies MS into subcategories and suggests appropriate treatment choices. It recommends treatment of RIS and CIS with poor prognostic factors. It largely equates the efficacy and safety of DMT with similar mechanisms of action or drug classes e.g. ocrelizumab is similar to rituximab. It allows early switching of treatment for unambiguous disease activity and those with progression independent of relapses. Autologous hematopoietic stem cell transplantation can be offered to patients who fail one high efficacy DMT. Pragmatic guidance on switching and stopping DMT, DMT choices in pregnancy, lactation and pediatric MS have been included. It is expected that these guidelines will be updated periodically as new data becomes available.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. You must be a paying subscriber if people want to ask questions unrelated to the Newsletters or Podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
X (Twitter) / LinkedIn / Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.








