




Does big data have the answers? The study below of over 27,000 people with multiple sclerosis (pwMS) and about 200,000 EDSS transitions tells us what we know already that relapses make only a small contribution to MS outcomes and this contribution is relatively early on in the disease. In other words, the real MS is smouldering MS or as measured in this study progression independent of relapses (PIRA).
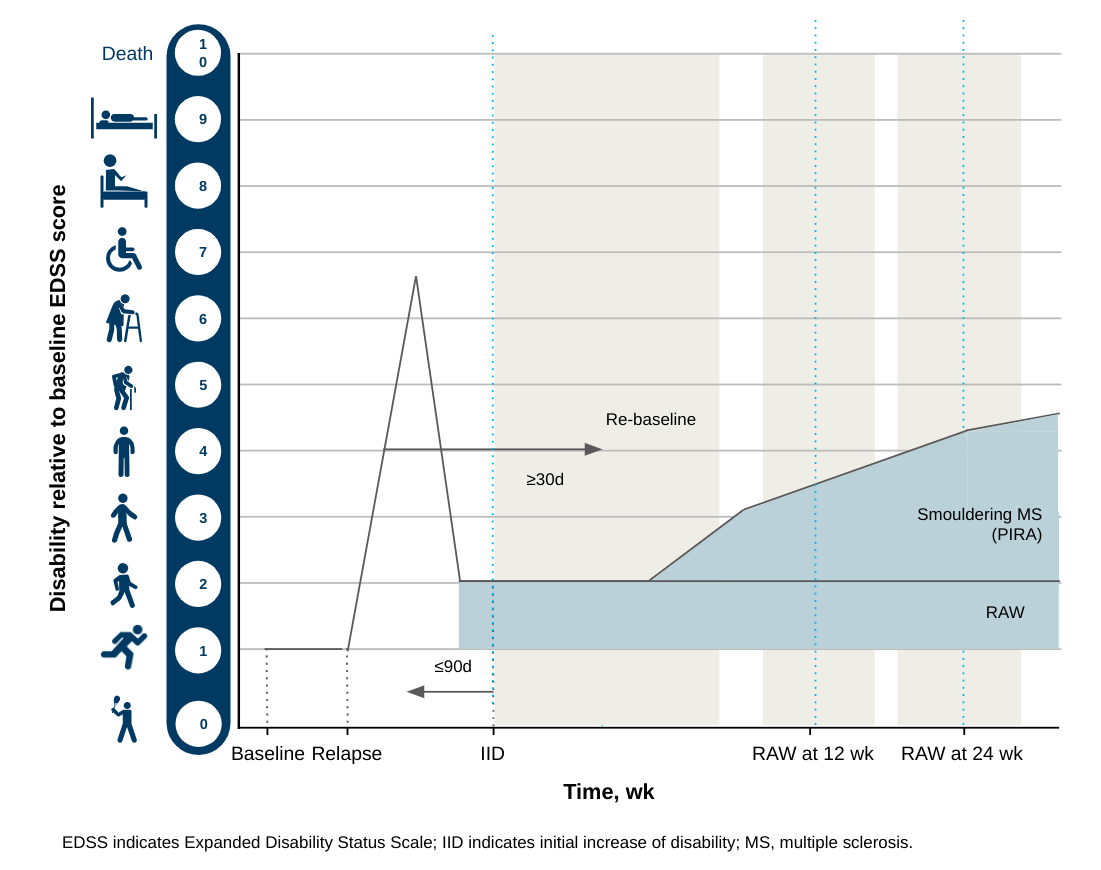
NOTE: Please remember that smouldering MS is more than PIRA. PIRA is what we can measure with the EDSS score (see figure below). Whereas smouldering MS refers to PIRA and other markers of ongoing end-organ damage, i.e. brain volume loss, grey matter loss, thalamic atrophy, slowly expanding lesions, raised neurofilament levels, cognitive decline, retinal nerve fibre layer thinning, worsening using neurological stress tests (walking distance, running speed, hand-eye coordination, balance tests, ….), etc….. It is important to realise that you can have a stable EDSS (no PIRA) and you can still be getting worse from smouldering MS. This is why I prefer the term smouldering MS to PIRA. Smouldering MS is so much more than PIRA.
Although the shows that following a year in which relapses occurred you are more likely to get worse. What they haven’t clearly stated is whether this was more pronounced in subjects on DMTs and did it also apply to study subjects on placebo. This point is critical because pre-existing data indicates this observation is limited to DMT-treated patients only, which implies that relapses are simply a biomarker of the DMT being suboptimal or ineffective in controlling the underlying MS disease process. The observation that relapses have little impact on outcome in placebo-treated or untreated patients tells us that relapses are not MS, but simply represent the immune system’s response to what is causing the disease.
YES, RELAPSES AND FOCAL MRI ACTIVITY ARE NOT MS.
I suspect that most pwMS will find it disappointing how modest the effect of MS disease-modifying treatments is on long-term MS outcomes. DMTs only delayed the time from EDSS 1 to 4 (walking problems) by ~3.5 years and time to EDSS 6.0 or a walking stick by ~3.1 years. As MS is a life-long disease these improvements in outcome are very disappointing and are a clear indication that we need to do more.
This data confirms that smouldering MS starts very early in the course of MS and is clearly the principal driver of disability accumulation. It also confirms that pre-existing disability and older age, both markers of reduced reserve capacity, and hence the ability to recover, are important risk factors for incomplete recovery from relapses. This tells us that relapse-associated worsening can’t be ignored and supports our treatment target of NEIDA (no evident inflammatory disease activity), but it is clear that we need to go beyond NEIDA and to focus on end-organ damage or smouldering disease.
It was reassuring to note that in paediatric MS the young and developing brain, which has a remarkable ability to recover function, acts as a buffer to smouldering disease. In children MS progression events independent of relapses are rare. This does not mean we should ignore smouldering MS in this population it is just harder to see clinically and when children with MS get older the biology of ageing still kicks in, it just takes longer to see the effects of ageing in younger people.
Overall this data supports applying the philosophy of marginal gains and the emphasis on the holistic management of MS to target brain health and anti-ageing strategies as an adjunct to managing smouldering MS.
This paper really dove-tails very well with our review on ‘Smouldering MS: the ‘real MS’ (Giovannoni et al. Ther Adv Neurol Disord 2022, Vol. 15: 1–18.), which I am thrilled about.

If you find the information in this Newsletter too complicated please read my earlier Newsletter on ‘Getting Worse’ and the holistic management of MS (MS-Selfie Newsletter, 2-July-2021). Please note the slides of our smouldering MS review are downloadable for you to use, distribute and hack. The more people who understand what is happening to their brains and spinal cords despite being on a DMT the better. Let’s hope the shift in emphasis to beyond-NEIDA means we may get more investment in MS research to tackle smouldering MS and to prevent MS.
Original Paper
Patients with multiple sclerosis acquire disability either through: (1) Relapse-associated worsening (RAW), or (2) progression independent of relapse activity (PIRA). This study addresses the relative contribution of relapses to disability worsening over the course of the disease, how early progression begins, and the extent to which multiple sclerosis therapies delay disability accumulation.
Using the Novartis-Oxford MS (NO.MS) data pool spanning all multiple sclerosis phenotypes and pediatric multiple sclerosis, we evaluated ∼200,000 EDSS transitions from >27,000 patients with ≤15 years follow-up. We analyzed three datasets: (A) A full analysis dataset containing all observational and randomized controlled clinical trials in which disability and relapses were assessed (N = 27,328); (B) All phase 3 clinical trials (N = 8364); and (C) All placebo-controlled phase 3 clinical trials (N = 4970). We determined the relative importance of RAW and PIRA, investigated the role of relapses on all-cause disability worsening using Andersen-Gill models, and observed the impact of the mechanism of worsening and disease modifying therapies (DMTs) on the time to reach milestone disability levels using time continuous Markov models.
PIRA started early in multiple sclerosis, occurred in all phenotypes, and became the principal driver of disability accumulation in the progressive phase of the disease. Relapses significantly increased the hazard of all-cause disability worsening events: Following a year in which relapses occurred (vs a year without relapses), the hazard increased by 31–48%; all p < 0.001. Pre-existing disability and older age were the principal risk factors for incomplete relapse recovery. For placebo-treated patients with minimal disability (EDSS 1) it took 8.95 years until increased limitation in walking ability (EDSS 4) and 18.48 years to require walking assistance (EDSS 6). Treating patients with DMTs delayed these times significantly by 3.51 years (95% confidence limit: 3.19, 3.96) and by 3.09 years (2.60, 3.72), respectively. In relapsing-remitting multiple sclerosis (RRMS), patients who worsened exclusively due to RAW events took a similar time to reach milestone EDSS values compared with those with PIRA events; the fastest transitions were observed in patients with PIRA and superimposed relapses.
Our data confirm relapses contribute to the accumulation of disability, primarily early in multiple sclerosis. PIRA starts already in RRMS and becomes the dominant driver of disability accumulation as the disease evolves. Pre-existing disability and older age are the principal risk factors for further disability accumulation. Using DMTs delays disability accrual by years, with the potential to gain time being highest in the earliest stages of multiple sclerosis.
Subscriptions
I am raising funds from paid subscriptions to administer the MS-Selfie Newsletter and associated MS-Selfie microsite that is currently in development. If you are an active paying subscriber thank you, your contribution is much appreciated.
Please note the money raised via subscriptions is being used to pay a professional medical writer to curate, rewrite and transfer the contents of the Newsletter onto a companion MS-Selfie microsite, which is being designed and maintained by a freelance web designer.
If you find these Newsletters helpful and want the wider MS community to continue to have access to all content I would encourage you to become a paid subscriber. Thank you.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust. The advice is intended as general advice and should not be interpreted as being personal clinical advice. If you have problems please tell your own healthcare professional who will be able to help you.








Share this post