



I don’t usually cover hardcore research and immunology on MS-Selfie. However, in the survey I did earlier this year, you specifically asked for research updates I surmised that you want to hear about basic research, particularly when it is potentially relevant to MS therapies and future MS research.

As you know, I am convinced that EBV is the cause of MS, so I am running a social media campaign under the hashtag #EBVcausesMS. Currently, there are two main competing theories of how EBV causes MS. On the one hand is the hit-and-run theory that EBV triggers autoimmunity through molecular mimicry, i.e. EBV fools the immune system into making an immune reaction against its proteins (e.g. EBNA-1) that cross-reacts with antigens in the central nervous system (CNS) which causes MS.
The second theory is that EBV is the driver of MS, and by continually cycling through its latent and lytic phases, it is responsible for driving MS pathology. This could either be by direct CNS infection, continuously stimulating autoreactive T and B cells, or upregulating a second virus such as MS-associated HERVs (human endogenous retroviruses), which in turn cause the damage. This latter is called the dual-viral hypothesis of MS.
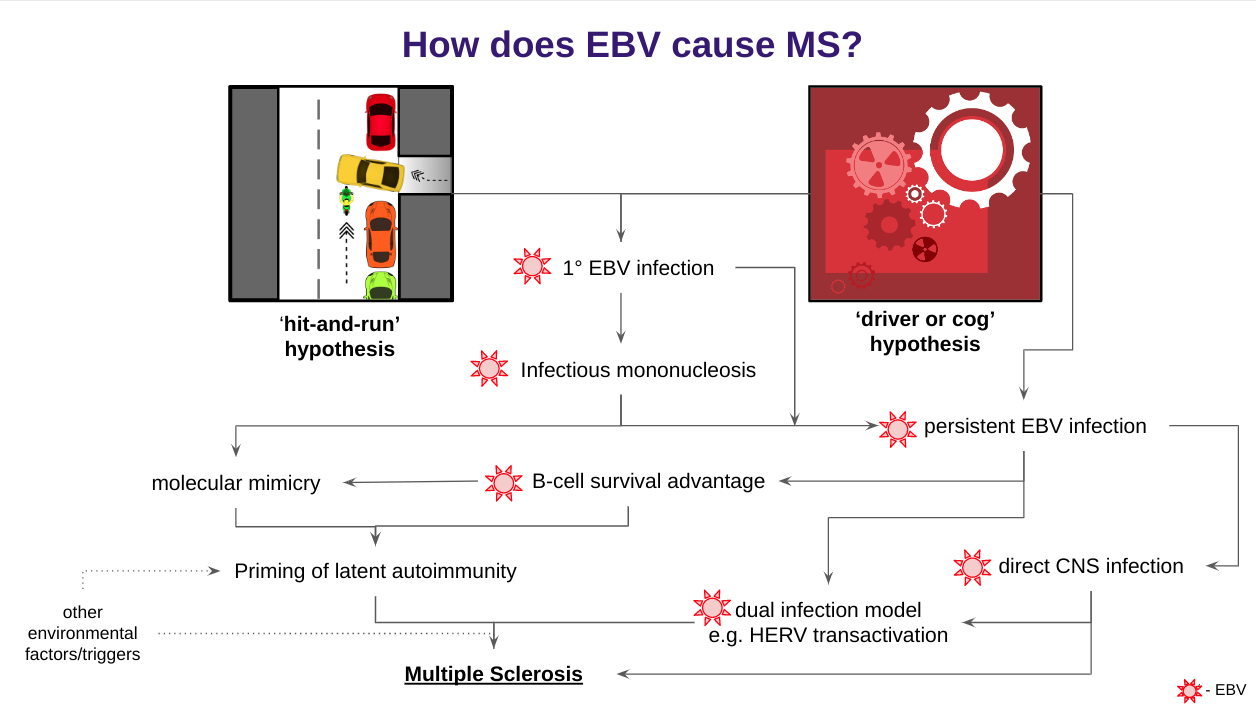
The observation that MS seems to respond to antiviral therapies that target EBV and retroviruses incidentally and to DMTs that affect EBV (lytic-latent cycling) supports direct EBV replication as a cause of MS and not the autoimmune molecular mimicry model. These are some of the main arguments for testing antiviral therapies in MS. The latest study below on EBV reactive T-cells supports the driver hypothesis (EBV replication) over the hit-and-run hypothesis.
When you first get exposed to EBV, your innate or hard-wired immune system responds to the virus to protect you from uncontrolled infection. The innate immune system is a holding system that recruits and helps your adaptive immune system to make a memory response so you can control the infection in the future. The adaptive immune system consists of B-cells that make antibodies (heat-seeking missiles) and T-cells (close combat). The T-cells are divided into CD8+ T-cells and CD4+ T-cells, which have different functions but can overlap.
A good analogy for the adaptive immune system is the military analogy. Innate immunity is a rapid reaction force, whereas the adaptive system consists of specialist units that come in after the battle begins. Antibodies are very specific and can travel long distances to their target, i.e. they act like heat-seeking or targeted missiles. T-cells are typically close combatants and need cell-cell contact. Once the immune system wins the initial battle, a subset of cells called central memory cells acts like a reconnaissance team that continually surveys the body for dissent action and are primed to respond and quell any rebellion as soon as it arises. Within this complex system are chains of commands with feedback loops to maximise the immune army's effectiveness to prevent collateral damage (friendly fire). Some people think the typical hot or acute MS lesion is due to collateral damage; as the immune system tries to deal with lytic EBV infection in the brain or spinal cord, the inflammatory mediators produced kill oligodendrocytes (myelin) and transect axons and kill nerve cells. This collateral damage results in relapse or new MRI lesions.
We have known for decades that people with MS and those at risk of getting MS have increased antibody levels and a greater variety of antibodies to many more EBV proteins than healthy controls. In other words, the MS immune system needs a wider range of long-range missiles to attack EBV. We don’t know why this happens, but it may be because pwMS can’t handle the EBV virus very well. I suspect that as EBV continuously reactivates itself from its latent or dormant phase, it keeps boosting antibody immune response to itself. An analogy for this would be booster vaccination, i.e. every time EBV reactivates, it boosts the immune system's response to itself, which drives the development of a wider and deeper antibody repertoire.
Antibodies are relatively easy to work with compared to T-cells. Previously, we used very laborious and time-consuming techniques to count the number of viral-specific T-cells and what viral antigens they respond to. Using these older technologies, there was a clear signal that pwMS had more EBV reactive T-cells against EBNA-1 (early EBV nuclear antigen-1) and more clones of cells responding to epitopes or places in the EBNA-1 protein compared to normal people or people with other diseases. In immunology jargon, this is referred to as having a wider T-cell repertoire to the virus. New technologies allow you to do these repertoire studies by simply sequencing T-cell receptors and using public databases to determine if that T-cell is reactive to EBV and to which protein it reacts. You can also now profile the type of T-cell by sequencing the mRNA or messages inside the cell using so-called single-cell methods.
Using this new repertoire analysis, the study below shows that pwMS have more EBV-specific T-cells than control subjects, including identical twins, where the twins who have MS have a wider repertoire compared to the twins who do not have MS. This twin comparison gets rid of most of the other genetic factors that may confound the interpretation of this data, which means that these results are real and likely to be very relevant to the pathogenesis of MS. Importantly, these T-cells reacted to both latent and lytic EBV antigens, suggesting that latent-lytic cycling likely boosts T-cell memory and diversity in pwMS and further strengthens the case for testing EBV antiviral agents in MS.
In this study, pwMS treated with natalizumab amplified this observation; i.e. they had a broad EBV reactive T-cell repertoire. Interferon-beta, a putative antiviral, and anti-CD20 treatment, which targets latent EBV in B-cells, did not modulate EBV-specific T-cells. The natalizumab data needs to be expanded and confirmed because it is so important.
Natalizumab does not deplete immune cells and simply traps them in the periphery. As natalizumab does not affect this T-cell response to EBV, it suggests this latent-lytic cycling continues unabated. This data does not tell whether this EBV latent-lytic cycling occurs within the CNS or peripheral compartment. EBV antigens from CNS lytic infection will reach the periphery via interstitial fluid and CSF outflow pathways and stimulate peripheral T and B-cell responses. We see the latter with the JC virus and PML (progressive multifocal leukoencephalopathy) in natalizumab-treated pwMS; a rising JCV antibody index or titre presages the overt development of PML.
The fact that interferon-beta does not affect these T-cell responses doesn’t say much, as interferon-beta is not a very effective DMT. In comparison, anti-CD20 therapy, which depletes latent EBV in memory B-cells and is a potent anti-inflammatory DMT ( suppressing relapses and new MRI lesions), doesn’t affect these T-cells responses. This suggests that latent-lytic EBV cycling occurs in a compartment not affected by anti-CD20 mediated B-cell depletion. Could this compartment be the CNS? I think, yes, anti-CD20 monoclonal antibodies penetrate the CNS poorly. This study supports the argument for using CNS-penetrant anti-EBV antivirals or anti-B-cell therapies. This is why drugs like cladribine, teriflunomide, proteasome inhibitors, BTK inhibitors, CNS penetrant anti-CD20 antibodies and other anti-virals are so exciting.
Finally, In healthy individuals, EBV-specific T cells were mainly effector-memory cells in peripheral blood and cerebrospinal fluid. In contrast, in pwMS, the cerebrospinal fluid also contained EBV-specific central-memory T cells. The latter suggests recent priming of these cells, i.e. they had recently seen EBV antigens, which in the case of CSF cells is likely to have taken place in the CNS.
In summary, this data is consistent with an ongoing anti-EBV immune reaction in MS and strongly suggests EBV latent-lytic cycling is a driving MS disease activity and that we need to start anti-viral studies as soon as possible. One could argue for using antivirals that work against both latent and lytic cycles. I have a dream of using just such an agent to treat MS, which will purge the body of EBV and cure MS. Am I being irresponsible in dreaming of curing MS? Many of my colleagues think so.
Please note we can also target EBV using antiviral or using immunotherapy. The latter could be via adoptive transfer of EBV-specific T-cells (e.g. Atara Bio or Tevogen), using an EBV vaccination to boost your immune responses to EBV (e.g. Moderna) or possibly by using an IRT (immune reconstitution therapy) such as AHSCT or alemtuzumab. The depletion-reconstitution cycle of an IRT may reduce EBV viral loads and rejuvenate jaded EBV T-cells responses that control the virus.
How many of you would be interested in participating in an add-on anti-EBV trial to test the hypothesis that EBV latent-lytic cycling drives MS disease activity?
Epstein-Barr virus (EBV) infection precedes multiple sclerosis (MS) pathology and cross-reactive antibodies might link EBV infection to CNS autoimmunity. As an altered anti-EBV T cell reaction was suggested in MS, we queried peripheral blood T cell receptor β chain (TCRβ) repertoires of 1,395 MS patients, 887 controls, and 35 monozygotic, MS-discordant twin pairs for multimer-confirmed, viral antigen-specific TCRβ sequences. We detected more MHC-I-restricted EBV-specific TCRβ sequences in MS patients. Differences in genetics or upbringing could be excluded by validation in monozygotic twin pairs discordant for MS. Anti-VLA-4 treatment amplified this observation, while interferon β- or anti-CD20 treatment did not modulate EBV-specific T cell occurrence. In healthy individuals, EBV-specific CD8+ T cells were of an effector-memory phenotype in peripheral blood and cerebrospinal fluid. In MS patients, cerebrospinal fluid also contained EBV-specific central-memory CD8+ T cells, suggesting recent priming. Therefore, MS is not only preceded by EBV infection, but also associated with broader EBV-specific TCR repertoires, consistent with an ongoing anti-EBV immune reaction in MS.
Subscriptions and donations
Paid subscriptions to MS-Selfie are being used to administer the Newsletter and associated MS-Selfie microsite currently in development. At the request of several readers, I have now added the option of making a one-off donation. To keep this initiative open to all readers, I would appreciate it if those who can afford a subscription, please subscribe. For active paying subscribers, thank you; your contribution is much appreciated.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust. The advice is general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.








Share this post