Definitely T1DM, although this is ‘autoimmune’ too. If I had that I would like an insulin syringe driver and continuous blood glucose monitor like the freestyle libre. In the next few years we’ll see these married into an automatic system which, once attached, removes the need to plan activities, insulin and meals in advance. Pancreatic implants are likely in the next decade. We’re just not so advanced in MS. MS treatment is in the dark ages compared to DM. To compare the pathologies the aetiologies are similar with the exception of end organ: Pancreas vs. Brain and spinal cord. I’d rather lose my pancreas. One day replacements will be available. That’s never going to happen for the CNS.
Totally agree that MS "treatment" is in the dark ages, as the "treatments" don't even "treat" MS-they simply reduce some manifestations of inflammatory disease. It's so sad that these "treatments" are so falsely and wrongly represented and "sold" to patients.
“As a thought experiment would you trade in MS for having T1DM or would you stick with the autoimmune disease you know already?”
Gladly swap MS for T1DM. Reasons: images of a post mortem MS brain; the impact of MS on mobility / walking (MS destroys the most simple of pleasures - game of tennis, stroll around an old city…..).
I’m answer to your question yes without any doubt I would swap my PPMS for T1DM. I would not wish my MS to the devil! A disease that is full of feet dragging and wait and see by much of the health services yourself excluded
If I was picking MS or TD1 I think I’d still pick having MS. When you’re relying on an external device to monitor and provide a critical hormone 24/7, the “will I accidentally die today?” odds are definitely worse than I would like. I would think the chance of sudden death due to MS is much lower, even with the TD1 management options that exist now.
I think this is an unfair question. Despite your long scientific explanation. As MSers we have enough judgement without having to rank our own MS experience. For those that think MS doesn’t end your life suddenly, it clearly can, be it via sepsis and pneumonia. 2 people are not having the same MS experience. I know my sister would have swapped her aggressive ms for a chance with T1DM. I’ve known several people die in their 60s with MS. And they suffered leading up to this. I also know people diagnosed young with T1DM who have lived well and others not.
What I do know is that MSers struggle to get the support they need. Don’t get calls returned when needing help. Continence advice can vary. Reason being as your general medic does not take on board the impact on our daily life’s. Oh, and we don’t drop down dead from it so we should be grateful.
Health is like a dartboard. You live with where the dart lands, if it’s bulls eye you get nothing only aging. and mostly try and make the most of it. It is unhelpful to be asked what is your preference, particularly with the nhs in such a volatile state. Another dartboard.
i can be in charge of whats happening (youre much more likely to be struck by lightning than have sudden unexpected T1DM death) . of course it helps that i dont have a sweet tooth.
but when you say "the vast majority of people with T1DM present with end-organ damage", that did jar with me. for T2DM , end organ damage surely usually means eyes , feet , other blood vessels - which only comes on with poorly controlled T1/T2DM. of course the pancreas has gone which is probly what you mean.
but its all manageable with current tech.
no sneaking up relapses / invisible smouldering and so on
I live with MS as well as six other autoimmune conditions, two of which are endocrine: Graves’ disease, which I’ve had since childhood and was treated with radioactive iodine, and Addison’s disease.
Living with Addison’s in particular has given me a much deeper appreciation for the severity of conditions like type 1 diabetes. While MS can make you feel awful and increase your susceptibility to infections due to treatment, the implications of a seemingly simple infection are on another level when you have Addison’s disease or T1DM. What might be minor for others can quickly become life-threatening if not managed appropriately.
I’ve experienced two adrenal crises in my life triggered by infection, and I would honestly trade any of my other conditions, including MS and lupus, not to have Addison’s. I strongly suspect I would feel the same way if I had T1DM.
Although MS often brings more visible physical limitations, conditions like Addison’s and T1DM come with very real, very frightening risks that can escalate rapidly and profoundly if not carefully managed at all times.
In this article, you write: "We can identify people with radiologically isolated syndrome (RIS), soon-to-be defined asymptomatic MS, albeit serendipitously at present, and then treat them to prevent them from developing clinically definite MS."
What is your evidence that treating those with RIS can "prevent them from developing clinically definite MS," as I am aware of the TERIS and the ARISE studies, neither of which found that treatment with "DMTs" prevented persons from developing clinically definite MS. Rather, what these studies found was that the "DMT" treatment resulted in reduced relative risk reductions vs placebo in preventing a first demyelinating event. In the TERIS study, presence of new or enlarging T2 lesion and new gadolinium-enhancing lesions were not found to differ between the DMT-treated and placebo-treated groups. Additionally: "Neither of these trials demonstrated a reduced disability long-term with DMT, although they were not powered to identify this, either" (source: Cleveland Clinic).
Your claim seems to be another exaggeration of claims made about the alleged efficacy of "DMTs" where the claims are not supported by evidence. I would like to see your evidence that supports your claim that "DMT" treatment can prevent people from developing CDMS, unless it is the TERIS and ARISE trials, which I am familiar with. If this is your evidence, it may be the case that "DMT" treatment possibly prevented SOME with RIS from going on to develop CDMS, but most definitely not at all, and then you get into details like NNT, etc, which I am not going to get into in more detail at this time.
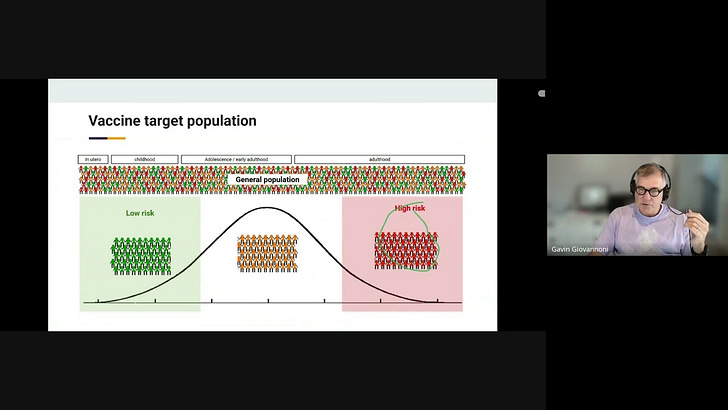
This is called secondary prevention, i.e. delaying someone with asymptomatic disease (RIS) from developing symptomatic disease (MS or CDMS). Again, this is semantics, but it is an important concept. Primary prevention refers to actions taken to prevent a disease from occurring in the first place (RIS or MS/CDMS), targeting healthy individuals in the general population. Finally, primordial prevention aims to avoid the emergence of risk factors. In the context of MS, this could be exposure to EBV.
The term "secondary prevention" is an absolute misrepresentative misnomer, then, because "delaying" something is NOT the same thing as "preventing" it. Again, this gives people false expectations, false hope, etc. Terrible.
When you have RIS and go on to have a clinical event, you are classified as having dissemination in time. To get into the trials, you had to have lesions on MRI (dissemination in space). Dissemination in time and space = CDMS. No exaggerated claims, only semantics. Based on the old definition of MS both teriflunomide and DMF delay the onset of MS. With the new criteria, many of those with RIS will now have MS. The new criteria eliminate the absolute requirement of having dissemination in time.
I would stick with MS just because I have had MS only for a few years, had Cladribine then Kesimpta and now will have HSCT at no cost in a few weeks. I also get monitored with regular Neurofilament light chain tests, brain volume measurements and neuropsychological testing. I don't have any physical disability I only have sensory symptoms such as some tingling and occasionally a little heat sensitivity. I don't have a large amount of lesions and probably had MS no longer than 5 years before diagnosis. So hoping the HSCT gives lifelong remission or at least enough remission until bi-specific T-cell engagers comes out with more add on neuroprotective and remyelination therapies as combination treatments
Gosh. Can I ask where you live ? HSCT and no physical disability? Is this unusual? I’m 6.5 on the EDS and get nothing but contradictory advice and empty hope. I really hope it works well for you. Doesn’t this show such a lottery in treatment though.
Luke - How have you managed to get all these tests (Neurofilament light chain tests, brain volume measurements and neuropsychological testing)? Where do you live?
It took me 10 yrs to get any treatment or support, so I’m amazed at how well you’re being monitored. And a little envious 😊. I feel fobbed off when I ask for those sorts of support.
I know this is off subject, but do you think mavenclad is an option for the 60 + crowd ?
Or too risky with targeting both B and T cells. I live in the USA and need to switch to a less costly form of dmt due to insurance limitations.
I don’t want permanent immune suppression.
Plus, now in progressive stage of MS.
I want to be able to take a btk medication if they become available this fall or winter…
This I one reason I’m not sure about aubagio, which takes years to clear out of your system. You’ve said in the past that what you take in the present could impact your future drug options…
You assert: “Cladribine, in my opinion, would be the best therapy for asymptomatic MS as it is a short course, relatively safe, well tolerated and has better efficacy than teriflunomide and DMF. “
However, per the information about Clinical Studies in the FDA labeling information for Mavenclad, teriflunomide, and DMF, Mavenclad performed no better than teriflunomide and DMF in these studies for the outcome of “Proportion of patients with 3-month EDSS progression.” Actually, Mavenclad performed worse, as there was no statistically significant difference found with Mavenclad (vs placebo) for the outcome of “Proportion of patients with 3-month EDSS progression.” However, in Study 1 for teriflunomide in the FDA labeling info, teriflunomide showed a statistically significant difference vs placebo for “Percent disability progression at week 108” for the 14mg dose and in Study 2, teriflunomide showed a statistically significant difference for the outcome of “Percent disability progression at week 108” for the 14mg dose (vs placebo). In Study 1 for Tecfidera in the FDA labeling information, there was a statistically significant (p=0.0050) difference between Tecfidera and placebo for the outcome of “Proportion with disability progression.”
When you assert that Mavenclad “has better efficacy” than teriflunomide and DMF, are you making this assertion based on the evidence that Mavenclad showed “better” evidence against relapses and MRI endpoints than teriflunomide and DMF? Why do you place so much emphasis on the endpoints of relapses/ARR and MRI endpoints in light of the above?
I think you should be more specific and transparent when you allege that Mavenclad “has better efficacy” than teriflunomide and DMT and state that Mavenclad’s “better efficacy” is only for the endpoints of relapses/ARR and MRI endpoints and NOT the disability progression endpoint, which is most likely the most important endpoint to MS patients and those who love them.
It is based on its effect on smouldering MS, i.e., CNS pathology, particularly CNS B-cells, brain volume loss, retinal nerve fibre thinning, slowly expanding lesions, CSF NFL levels, CSF oligoclonal bands, free lambda and kappa light chain levels, and the long-term follow-up of patients. The ORACLE CIS trial data is very impressive, with over 50% of treated patients not needing treatment after 10 years. We also have some good open-label data on its impact in patients with more advanced disease, which underpins our CHARIOT-MS trial in advanced MS targeting upper limb function.
The question is whether any, some, or all of the biomarkers, MRI findings, etc that you mention that Mavenclad shows efficacy against have a meaningful result in terms of disability progression. There are too many for me to get into now, but, for example, in the HERCULES results for tolebrutinib, it was found that tolebrutinb showed a 31% relative risk reduction for 6 month CDP vs placebo (NNT of around 12, though, which is far from impressive) but did not affect brain volume loss, which calls into question whether BVL contributes to progression in MS. This is just one example that I can offer for now with limited time.
Regarding the CHARIOT-MS trial along with the Ocrevus trial assessing upper limb function, I am curious as to why there are trials specifically evaluating upper limb function in particular, as upper limb function is assessed by EDSS such as in the pyramidal and cerebellar categories in terms of extremeties. Is it because upper limb function is considered "low hanging fruit," essentially? That the thinking is that it would be the easiest "area" to assess to say that a given "DMT" shows efficacy? Something doesn't add up to me about the emphasis on upper limb function in these trials to me.
When you have lost the function of your legs and are in a wheelchair, your hands become your legs. That is why there is a focus on hand function in advanced MS. I can only assume you are not a wheelchair user.
You have a lot to learn about MS. I wouldn't rely on the regulators. They are tied to the EDSS and are decades behind the rest of the field. I suggest you start with length dependency and therapeutic lag.


Definitely T1DM, although this is ‘autoimmune’ too. If I had that I would like an insulin syringe driver and continuous blood glucose monitor like the freestyle libre. In the next few years we’ll see these married into an automatic system which, once attached, removes the need to plan activities, insulin and meals in advance. Pancreatic implants are likely in the next decade. We’re just not so advanced in MS. MS treatment is in the dark ages compared to DM. To compare the pathologies the aetiologies are similar with the exception of end organ: Pancreas vs. Brain and spinal cord. I’d rather lose my pancreas. One day replacements will be available. That’s never going to happen for the CNS.
Totally agree that MS "treatment" is in the dark ages, as the "treatments" don't even "treat" MS-they simply reduce some manifestations of inflammatory disease. It's so sad that these "treatments" are so falsely and wrongly represented and "sold" to patients.
“As a thought experiment would you trade in MS for having T1DM or would you stick with the autoimmune disease you know already?”
Gladly swap MS for T1DM. Reasons: images of a post mortem MS brain; the impact of MS on mobility / walking (MS destroys the most simple of pleasures - game of tennis, stroll around an old city…..).
I’m answer to your question yes without any doubt I would swap my PPMS for T1DM. I would not wish my MS to the devil! A disease that is full of feet dragging and wait and see by much of the health services yourself excluded
If I was picking MS or TD1 I think I’d still pick having MS. When you’re relying on an external device to monitor and provide a critical hormone 24/7, the “will I accidentally die today?” odds are definitely worse than I would like. I would think the chance of sudden death due to MS is much lower, even with the TD1 management options that exist now.
This is a stupid question? We want neither .
I think this is an unfair question. Despite your long scientific explanation. As MSers we have enough judgement without having to rank our own MS experience. For those that think MS doesn’t end your life suddenly, it clearly can, be it via sepsis and pneumonia. 2 people are not having the same MS experience. I know my sister would have swapped her aggressive ms for a chance with T1DM. I’ve known several people die in their 60s with MS. And they suffered leading up to this. I also know people diagnosed young with T1DM who have lived well and others not.
What I do know is that MSers struggle to get the support they need. Don’t get calls returned when needing help. Continence advice can vary. Reason being as your general medic does not take on board the impact on our daily life’s. Oh, and we don’t drop down dead from it so we should be grateful.
Health is like a dartboard. You live with where the dart lands, if it’s bulls eye you get nothing only aging. and mostly try and make the most of it. It is unhelpful to be asked what is your preference, particularly with the nhs in such a volatile state. Another dartboard.
id much rather have T1DM!
i can be in charge of whats happening (youre much more likely to be struck by lightning than have sudden unexpected T1DM death) . of course it helps that i dont have a sweet tooth.
but when you say "the vast majority of people with T1DM present with end-organ damage", that did jar with me. for T2DM , end organ damage surely usually means eyes , feet , other blood vessels - which only comes on with poorly controlled T1/T2DM. of course the pancreas has gone which is probly what you mean.
but its all manageable with current tech.
no sneaking up relapses / invisible smouldering and so on
Thank you for raising this topic, Prof G.
I live with MS as well as six other autoimmune conditions, two of which are endocrine: Graves’ disease, which I’ve had since childhood and was treated with radioactive iodine, and Addison’s disease.
Living with Addison’s in particular has given me a much deeper appreciation for the severity of conditions like type 1 diabetes. While MS can make you feel awful and increase your susceptibility to infections due to treatment, the implications of a seemingly simple infection are on another level when you have Addison’s disease or T1DM. What might be minor for others can quickly become life-threatening if not managed appropriately.
I’ve experienced two adrenal crises in my life triggered by infection, and I would honestly trade any of my other conditions, including MS and lupus, not to have Addison’s. I strongly suspect I would feel the same way if I had T1DM.
Although MS often brings more visible physical limitations, conditions like Addison’s and T1DM come with very real, very frightening risks that can escalate rapidly and profoundly if not carefully managed at all times.
In this article, you write: "We can identify people with radiologically isolated syndrome (RIS), soon-to-be defined asymptomatic MS, albeit serendipitously at present, and then treat them to prevent them from developing clinically definite MS."
What is your evidence that treating those with RIS can "prevent them from developing clinically definite MS," as I am aware of the TERIS and the ARISE studies, neither of which found that treatment with "DMTs" prevented persons from developing clinically definite MS. Rather, what these studies found was that the "DMT" treatment resulted in reduced relative risk reductions vs placebo in preventing a first demyelinating event. In the TERIS study, presence of new or enlarging T2 lesion and new gadolinium-enhancing lesions were not found to differ between the DMT-treated and placebo-treated groups. Additionally: "Neither of these trials demonstrated a reduced disability long-term with DMT, although they were not powered to identify this, either" (source: Cleveland Clinic).
Your claim seems to be another exaggeration of claims made about the alleged efficacy of "DMTs" where the claims are not supported by evidence. I would like to see your evidence that supports your claim that "DMT" treatment can prevent people from developing CDMS, unless it is the TERIS and ARISE trials, which I am familiar with. If this is your evidence, it may be the case that "DMT" treatment possibly prevented SOME with RIS from going on to develop CDMS, but most definitely not at all, and then you get into details like NNT, etc, which I am not going to get into in more detail at this time.
Frustrating...
This is called secondary prevention, i.e. delaying someone with asymptomatic disease (RIS) from developing symptomatic disease (MS or CDMS). Again, this is semantics, but it is an important concept. Primary prevention refers to actions taken to prevent a disease from occurring in the first place (RIS or MS/CDMS), targeting healthy individuals in the general population. Finally, primordial prevention aims to avoid the emergence of risk factors. In the context of MS, this could be exposure to EBV.
The term "secondary prevention" is an absolute misrepresentative misnomer, then, because "delaying" something is NOT the same thing as "preventing" it. Again, this gives people false expectations, false hope, etc. Terrible.
https://www.iwh.on.ca/what-researchers-mean-by/primary-secondary-and-tertiary-prevention
When you have RIS and go on to have a clinical event, you are classified as having dissemination in time. To get into the trials, you had to have lesions on MRI (dissemination in space). Dissemination in time and space = CDMS. No exaggerated claims, only semantics. Based on the old definition of MS both teriflunomide and DMF delay the onset of MS. With the new criteria, many of those with RIS will now have MS. The new criteria eliminate the absolute requirement of having dissemination in time.
Your thoughts on reclassifying RIS as MS are intriguing. Where do you see CIS fitting in?
CIS is already MS in the vast majority of cases.
I would stick with MS just because I have had MS only for a few years, had Cladribine then Kesimpta and now will have HSCT at no cost in a few weeks. I also get monitored with regular Neurofilament light chain tests, brain volume measurements and neuropsychological testing. I don't have any physical disability I only have sensory symptoms such as some tingling and occasionally a little heat sensitivity. I don't have a large amount of lesions and probably had MS no longer than 5 years before diagnosis. So hoping the HSCT gives lifelong remission or at least enough remission until bi-specific T-cell engagers comes out with more add on neuroprotective and remyelination therapies as combination treatments
Gosh. Can I ask where you live ? HSCT and no physical disability? Is this unusual? I’m 6.5 on the EDS and get nothing but contradictory advice and empty hope. I really hope it works well for you. Doesn’t this show such a lottery in treatment though.
Luke - How have you managed to get all these tests (Neurofilament light chain tests, brain volume measurements and neuropsychological testing)? Where do you live?
It took me 10 yrs to get any treatment or support, so I’m amazed at how well you’re being monitored. And a little envious 😊. I feel fobbed off when I ask for those sorts of support.
I know this is off subject, but do you think mavenclad is an option for the 60 + crowd ?
Or too risky with targeting both B and T cells. I live in the USA and need to switch to a less costly form of dmt due to insurance limitations.
I don’t want permanent immune suppression.
Plus, now in progressive stage of MS.
I want to be able to take a btk medication if they become available this fall or winter…
This I one reason I’m not sure about aubagio, which takes years to clear out of your system. You’ve said in the past that what you take in the present could impact your future drug options…
Thank you for the vital info that you provide!
You assert: “Cladribine, in my opinion, would be the best therapy for asymptomatic MS as it is a short course, relatively safe, well tolerated and has better efficacy than teriflunomide and DMF. “
However, per the information about Clinical Studies in the FDA labeling information for Mavenclad, teriflunomide, and DMF, Mavenclad performed no better than teriflunomide and DMF in these studies for the outcome of “Proportion of patients with 3-month EDSS progression.” Actually, Mavenclad performed worse, as there was no statistically significant difference found with Mavenclad (vs placebo) for the outcome of “Proportion of patients with 3-month EDSS progression.” However, in Study 1 for teriflunomide in the FDA labeling info, teriflunomide showed a statistically significant difference vs placebo for “Percent disability progression at week 108” for the 14mg dose and in Study 2, teriflunomide showed a statistically significant difference for the outcome of “Percent disability progression at week 108” for the 14mg dose (vs placebo). In Study 1 for Tecfidera in the FDA labeling information, there was a statistically significant (p=0.0050) difference between Tecfidera and placebo for the outcome of “Proportion with disability progression.”
Mavenclad performed well for the outcomes of ARR and MRI Endpoints, but research has shown that there is no association between relapses and long-term progression or CDW (https://www.genentech-medinfo.com/content/dam/gene/genentech-medinfo/pdfs/disease-progression-in-ms.pdf?fbclid=IwY2xjawKl8BRleHRuA2FlbQIxMQABHjHqgmjhiH8FA_qwiU-Hbs4MAuA8anAs8gvvb6-CNrbfpgMNFofwJPmjaufS_aem_X39EBKpjmb6x5i3XyP0yLw). Research has also only shown a weak to moderate association between progression and lesions in MS (I am happy to provide the sources for this assertion upon request).
When you assert that Mavenclad “has better efficacy” than teriflunomide and DMF, are you making this assertion based on the evidence that Mavenclad showed “better” evidence against relapses and MRI endpoints than teriflunomide and DMF? Why do you place so much emphasis on the endpoints of relapses/ARR and MRI endpoints in light of the above?
I think you should be more specific and transparent when you allege that Mavenclad “has better efficacy” than teriflunomide and DMT and state that Mavenclad’s “better efficacy” is only for the endpoints of relapses/ARR and MRI endpoints and NOT the disability progression endpoint, which is most likely the most important endpoint to MS patients and those who love them.
Again, very frustrating and discouraging to see.
It is based on its effect on smouldering MS, i.e., CNS pathology, particularly CNS B-cells, brain volume loss, retinal nerve fibre thinning, slowly expanding lesions, CSF NFL levels, CSF oligoclonal bands, free lambda and kappa light chain levels, and the long-term follow-up of patients. The ORACLE CIS trial data is very impressive, with over 50% of treated patients not needing treatment after 10 years. We also have some good open-label data on its impact in patients with more advanced disease, which underpins our CHARIOT-MS trial in advanced MS targeting upper limb function.
The question is whether any, some, or all of the biomarkers, MRI findings, etc that you mention that Mavenclad shows efficacy against have a meaningful result in terms of disability progression. There are too many for me to get into now, but, for example, in the HERCULES results for tolebrutinib, it was found that tolebrutinb showed a 31% relative risk reduction for 6 month CDP vs placebo (NNT of around 12, though, which is far from impressive) but did not affect brain volume loss, which calls into question whether BVL contributes to progression in MS. This is just one example that I can offer for now with limited time.
Regarding the CHARIOT-MS trial along with the Ocrevus trial assessing upper limb function, I am curious as to why there are trials specifically evaluating upper limb function in particular, as upper limb function is assessed by EDSS such as in the pyramidal and cerebellar categories in terms of extremeties. Is it because upper limb function is considered "low hanging fruit," essentially? That the thinking is that it would be the easiest "area" to assess to say that a given "DMT" shows efficacy? Something doesn't add up to me about the emphasis on upper limb function in these trials to me.
When you have lost the function of your legs and are in a wheelchair, your hands become your legs. That is why there is a focus on hand function in advanced MS. I can only assume you are not a wheelchair user.
You have a lot to learn about MS. I wouldn't rely on the regulators. They are tied to the EDSS and are decades behind the rest of the field. I suggest you start with length dependency and therapeutic lag.
https://gavingiovannoni.substack.com/p/is-your-ms-salvageable