


Yo-yoing comes at a price
Are you a yo-yoer, i.e. someone who loses and gains weight in cycles?

Are you a yo-yoer, i.e. someone who loses and gains weight in cycles?

This time of year is when many people decide to go on a diet and lose weight. It has now emerged that people who yo-yo with their weight are more likely to lose muscle mass and become sarcopenic. Several studies have shown that caloric restriction and intermittent fasting diets are associated with loss of muscle mass. This occurs because you need to break down muscle to release protein to make glucose via the metabolic process called gluconeogenesis. This is less likely to happen on a low-carbohydrate-high-protein or ketogenic diet.
Sarcopenia (loss of muscle mass) becomes a problem over time. Each round of weight loss and weight gain combined with other potential complications of having MS, i.e. reduced mobility and exercise, corticosteroid exposure, early ageing, and chronic inflammation exacerbates sarcopenia. People with MS, particularly advanced MS, are known to have a higher incidence of sarcopenia (see paper below). This is a problem because sarcopenia is an independent risk factor for frailty (reduced resilience), morbidity and mortality.
Over the last few years, I have seen an increasing number of pwMS on extreme diets with profound sarcopenia. None of these patients are well. As I am writing this, several patients come to mind who have very low BMIs (body mass index), are clearly frail and are either having falls or at high risk of falls. I have referred some of these patients to dieticians to try to address their sarcopenia.
The diet to prevent or treat sarcopenia must have adequate protein, as it's crucial for muscle maintenance and growth. The recommended dietary allowance (RDA) for protein is ~0.8 grams per kilogram of body weight per day, but pwMS and older adults or those at risk for sarcopenia benefit from higher levels. It is important to ensure your protein intake is high-quality and includes a variety of protein sources, such as lean meats, poultry, fish, eggs, dairy products, legumes, and soy products. It is also essential to ensure you get adequate vitamins and minerals. Regular exercise, including resistance training, such as weight lifting, is important to build and maintain muscle mass.
So please go gently with your weight loss programmes this year so as not to lose too much weight too quickly at the expense of your muscle mass and general health. Yes, #MuscleHealth is yet another thing for pwMS to be aware of.
How many of you know if you have sarcopenia? The following is the so-called SARC-F scale.
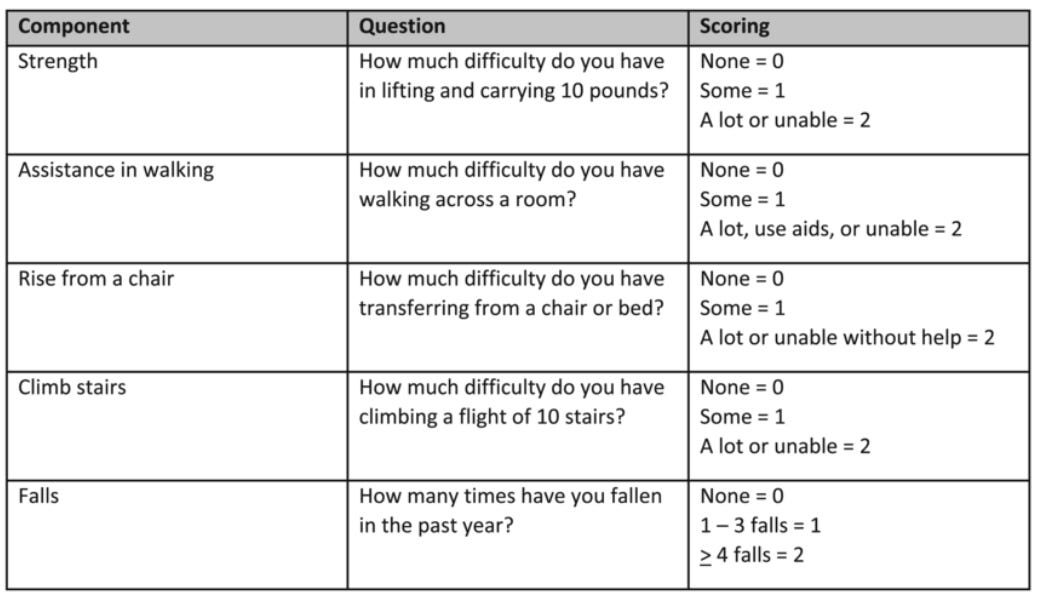
A SARC-F score of >=4 indicates that you need a more comprehensive assessment for sarcopenia. Please note this score is used in the elderly and has not been validated in pwMS.
I am interested in knowing how many of you have had your muscle mass assessed and how many of you yo-yo diet.
The following is some general information about sarcopenia that is not only for pwMS.
So, what is sarcopenia?
Sarcopenia is a condition characterised by the loss of skeletal muscle mass and strength, typically as part of the ageing process. Sarcopenia can affect an individual's functional status and quality of life, leading to a higher risk of falls, frailty, and dependency.

Causes and Risk Factors
Ageing: The primary cause of sarcopenia is ageing. As people age, there is a natural decline in muscle mass and strength.
Reduced physical activity: a sedentary lifestyle contributes significantly to the development of sarcopenia. Lack of exercise leads to faster muscle loss.
Inadequate nutrition: poor nutrition, especially insufficient protein intake, can accelerate muscle loss. As people age, their nutritional requirements may change, and their appetite may decrease.
Hormonal changes: changes in hormone levels with age, such as reduced growth hormone, testosterone, and oestrogen, can contribute to muscle loss.
Neuromuscular degeneration: the decline in the quality and quantity of motor neurons that control muscle movements leads to muscle wasting atrophy.
Chronic diseases: conditions like cancer, heart failure, and chronic kidney disease can exacerbate muscle loss.
Inflammation: chronic low-level inflammation, which can increase with age, is also thought to contribute to muscle degradation. This includes chronic gum disease, urinary tract infections, pressure sores and chest infections.
Consequences
Increased risk of falls and fractures: muscle weakness and loss of balance associated with sarcopenia can lead to a higher risk of falls, increasing the risk of fractures.
Physical disability: loss of muscle mass can lead to difficulties performing daily activities, reducing independence and quality of life.
Frailty: sarcopenia is a major component of frailty, a condition characterised by decreased physiological reserves and increased vulnerability to stressors.
Metabolic disorders: sarcopenia can contribute to the development of metabolic disorders, such as insulin resistance and type 2 diabetes, due to the role of muscle in glucose metabolism.
Increased mortality: severe sarcopenia is associated with an increased risk of mortality, primarily due to complications like falls, fractures, and the worsening of chronic diseases.
Management and Prevention
Regular exercise: resistance training and aerobic exercises are effective in preventing and managing sarcopenia.
Adequate nutrition: ensuring sufficient protein intake and a balanced diet rich in vitamins and minerals is crucial.
Lifestyle modifications: maintaining an active lifestyle, avoiding smoking, and limiting alcohol consumption can help.
Management of chronic diseases: effectively managing conditions like diabetes and heart disease can mitigate their impact on muscle health.
Hormonal replacement therapy: HRT might be considered.
Early recognition and intervention are key in managing sarcopenia. Regular physical activity and proper nutrition are the cornerstones of prevention and treatment. As the condition is closely linked to ageing, a holistic approach that includes regular health check-ups and addressing multiple aspects of health is beneficial.
Research paper
Background: The relation of sarcopenia and disability in MS is unknown.
Objective: To investigate the relation of temporal muscle thickness (TMT) and disability.
Methods: A cohort of 132 people who presented with a clinically isolated syndrome (CIS) suggestive of MS at a mean age of 30.0 years, were prospectively followed clinically and with MRI over 30-years. TMT and expanded disability status scale (EDSS) were assessed at baseline, one- five- ten- fourteen- twenty- and thirty-year follow-up.
Results: At 30-years, 27 participants remained classified as having had a CIS, 34 converted to relapsing remitting MS, 26 to secondary progressive MS, and 16 had died due to MS. Using linear mixed effect models with subject nested in time, greater annualized TMT-thinning was seen in individuals who developed MS (-0.04 mm/a, 95%CI: -0.07 to -0.01, p = 0.023). In those who converted to MS, a thinner TMT was reached at 14- (p = 0.008), 20- (p = 0.002) and 30-years (p< 0.001). TMT was negatively correlated with EDSS at 20-years (R=-0.18, p = 0.032) and 30-years (R-0.244, p = 0.005). Longitudinally, TMT at earlier timepoints was not predictive for 30-year clinical outcomes.
Conclusion: TMT thinning is accelerated in MS and correlated with disability in later disease stages, but is not predictive of future disability.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. If people want to ask questions unrelated to the Newsletters or Podcasts, you must be a paying subscriber. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
X (Twitter) / LinkedIn / Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.
No to yo-yo-ing. I do IF (12:12) and aim to eat 1g of protein for every kg of body weight at minimum per day. Diet is high in protein and very low in carbs - though not strictly keto by design. Weight lift 5 days per week and workout every day to retain strength and actively build muscle. Have seen significant muscle gains since starting this 8 months ago. (And I am lost-menopausal)
I've never had a muscle mass assessment. I score 6 points the SARC-F scale.