


Will CD19-targeted CAR T-cell therapy cure MS?
Who is right; the naysayers saying CAR T-cells are too risky, or those of us who want to press ahead with CD-19-targeted CAR T-cell therapies in MS?

I increasingly get pushback from my colleagues, MS charities and other MS stakeholders about using the C-word, i.e. multiple sclerosis is a curable disease. I am not trying to be alarmist or raise false expectations when I say MS is a curable disease (see ‘To cure or not to cure MS, that is the question’, 24-Aug-2023). I claim MS is a curable disease because of what I have seen happen to some of my patients who have been treated early with alemtuzumab and from other case studies of patients treated with AHSCT. Then, there is a scientific perspective on what causes MS. I was convinced decades ago that EBV is the cause of MS. This was based on my interpretation of data published in the literature, which has only become stronger over time. It is now clear that EBV is necessary but not sufficient for someone to develop MS.
Those of us who are interested in curing MS argue about how EBV causes MS. There are currently four leading EBV causation theories. (1) EBV triggers autoimmunity as a hit-and-run event, and the virus doesn’t play a role in the disease after the initial triggering event. (2) EBV-infected B-cells are responsible for driving autoimmunity by presenting auto-antigens, and these cells persist because of latent EBV infection. (3) Active EBV infection, i.e. latent-lytic cycling, drives MS disease activity. The latter could be in the CNS or the periphery, such as deep cervical lymph nodes. (4) EBV causes MS by transactivating HERVs (human endogenous retroviruses), which are responsible for triggering and maintaining an autoimmune response. The important thing is that these hypotheses are testable or falsifiable with different experiments.
Two proposed experiments target latent and lytic EBV infection with antivirals or immunotherapy. The former is to either control EBV replication or to use antiviral strategies to purge the body of the virus. Conversely, immunotherapy aims to boost the exhausted T-cell response so that one’s own immune system controls the virus.
In 2015, we hypothesised that CD19-targeted CAR T-cells would be one form of immunotherapy that would purge the body of EBV-infected B-cells. These cells are engineered to find and kill any cell expressing CD19. This includes most B-cells and some plasmablasts. The advantage CAR T-cells have over B-cell targeting monoclonal antibodies (anti-CD20 or anti-CD19) and the new generation bispecific antibodies (anti-CD3/CD20) is that they traffic into the CNS. I think it is important to scrub the central nervous system (CNS) clean of pathogenic B-cells, plasmablasts, and other hard-to-reach B-cell niches that may harbour EBV-infected B-cells.
I have spent the better two years trying to get CAR T-cell companies interested in MS. The good news is that three phase-1 CAR T-cell safety studies will be starting in MS, with several other companies planning to explore this technology in MS as well. I was, therefore, thrilled to read the article below in this week’s NEJM, showing that the responses of other autoimmune diseases to CD19-targeted CAR T-cells are durable. The treatment effect is so durable that the accompanying editorial discussed the possibility that these subjects have been cured of their autoimmune diseases.
Despite this evidence and the scientific rationale, we have a battle on our hands to test CAR T-cells in MS. Many of my colleagues feel that this therapy is too risky for pwMS. They argue that when we have such effective licensed treatments for MS, can we justify exposing patients to the risks associated with CAR T-cell therapies? My counter-argument is that our current therapies are not that effective in treating MS, which is why we need to explore alternative hypotheses and treatments. Who is right; the naysayers saying CAR T-cells are too risky, or those of us who want to press ahead with CD-19-targeted CAR T-cell therapies in MS?
Knowing what you know about MS and its possible cause, would you be willing to volunteer for a CD-19-targeted CAR T-cell trial?
You may find my recent MS-Selfie Newsletter on CAR T-cells helpful for more background information.
AHSCT vs. CAR T-cells to treat MS: Do we have to use AHSCT as an immunological sledgehammer to treat MS? Can't we use something simpler like a targeted immunotherapy or an antiviral to control EBV? (2-Dec-2023)
NEJM Article
BACKGROUND: Treatment for autoimmune diseases such as systemic lupus erythematosus (SLE), idiopathic inflammatory myositis, and systemic sclerosis often involves long-term immune suppression. Resetting aberrant autoimmunity in these diseases through deep depletion of B cells is a potential strategy for achieving sustained drug-free remission.
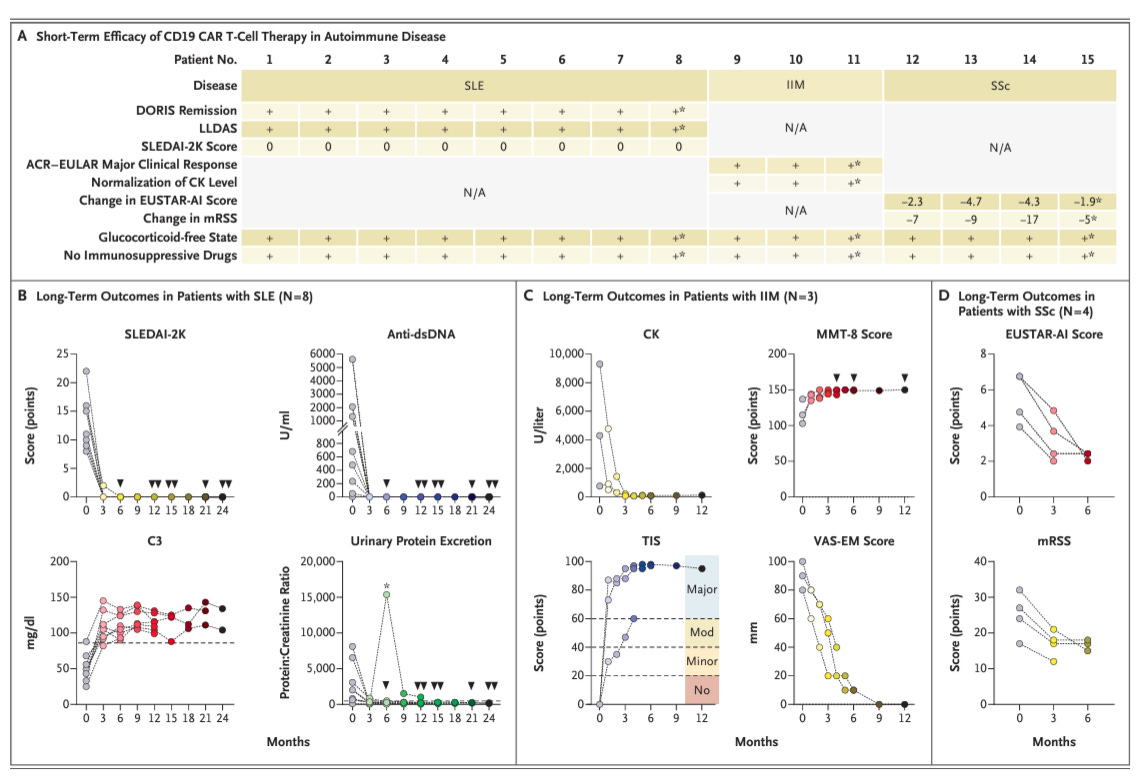
METHODS: We evaluated 15 patients with severe SLE (8 patients), idiopathic inflammatory myositis (3 patients), or systemic sclerosis (4 patients) who received a single infusion of CD19 chimeric antigen receptor (CAR) T cells after preconditioning with fludarabine and cyclophosphamide. Efficacy up to 2 years after CAR T-cell infusion was assessed by means of Definition of Remission in SLE (DORIS) remission criteria, American College of Rheumatology–European League against Rheumatism (ACR–EULAR) major clinical response, and the score on the European Scleroderma Trials and Research Group (EUSTAR) activity index (with higher scores indicating greater disease activity), among others. Safety variables, including cytokine release syndrome and infections, were recorded.
RESULTS: The median follow-up was 15 months (range, 4 to 29). The mean (±SD) duration of B-cell aplasia was 112±47 days. All the patients with SLE had DORIS remission, all the patients with idiopathic inflammatory myositis had an ACR–EULAR major clinical response, and all the patients with systemic sclerosis had a decrease in the score on the EUSTAR activity index. Immunosuppressive therapy was completely stopped in all the patients. Grade 1 cytokine release syndrome occurred in 10 patients. One patient each had grade 2 cytokine release syndrome, grade 1 immune effector cell–associated neurotoxicity syndrome, and pneumonia that resulted in hospitalization.
CONCLUSIONS: In this case series, CD19 CAR T-cell transfer appeared to be feasible, safe, and efficacious in three different autoimmune diseases, providing rationale for further controlled clinical trials. (Funded by Deutsche Forschungsgemeinschaft and others.)
Editorial
Isaacs. CAR T Cells — A New Horizon for Autoimmunity? N Engl J Med 2024; 390:758-759.
…. “Could CAR T-cell therapy cure autoimmunity? Such cure will require eradication of relevant immune memory from both B-cell and T-cell compartments.5 B cells that reconstitute blood after treatment resemble a naïve repertoire, with loss of some autoimmunity-associated characteristics. If disease-associated clones have been eradicated, disease recurrence will require their stochastic regeneration and subsequent activation, also requiring cognate T-cell “help.” This interaction is reciprocal, with B cells concurrently activating T cells. Consequently, deep B-cell depletion could cause secondary loss of autoreactive T cells by “neglect,” although some memory T cells are likely to persist. This scenario has further oncologic parallels, in which relapse probability could be determined by the presence or absence of “minimal residual disease.” However, such a concept is an oversimplification and neglects intricacies of our immune system, such as the existence of CD19-expressing regulatory B cells that protect against autoimmunity….”
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. You must be a paying subscriber if people want to ask questions unrelated to the Newsletters or Podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
X (Twitter) / LinkedIn / Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.
I’d certainly volunteer for CAR-T trials. There are currently few, if any, drugs or treatments that seem to make a real difference in secondary progressive MS - so it’s worth finding out whether CAR-T therapy would or could help - or even potentially cure - MS. Anyone who thinks that SPMS is not ‘bad’ enough to warrant the risks of taking part in any trials has clearly not had to live through decades with a chronic illness that progressively eats away at our lives and our hopes. So many illnesses that we once thought of as hopeless or incurable are now either curable or at least modifiable. We are very lucky to be living in an amazing era for medical breakthroughs. We will be able to do so much more for people with MS if we can somehow manage to tailor those scientific breakthroughs to treat or modify this ghastly disease.
I made a Facebook group for patients undergoig CAR-T treatment for autoimmune illness.
Some of te members have already had CAR-T done in Germany, USA, and China.
So please join the group
https://www.facebook.com/groups/cartautoimmune