


We have a winner: crossword #2 results
Twenty-two people completed last week's crossword correctly and my random number generator has selected the winner. This newsletter covers some of the problems pwMS have after having optic neuritis.

Did you know that more than half of people with established multiple sclerosis (pwMS) have had an episode of optic neuritis (an MS lesion in the optic nerve)? Not all episodes of optic neuritis cause symptoms and can be subclinical. We can detect the latter using visual evoked potentials that show slowed conduction in a particular optic nerve or more sensitive visual tests or visual stress tests.

When optic neuritis recovers the conduction speed of nerve impulses travelling through the recovered nerve rarely gets back to normal and is slower than the conduction speed in the unaffected eye. In addition, the conduction speed can change depending on fatigue or ambient temperature changes. The conduction in the affected, but remyelinated, nerves can even fail and this is can result in intermittent blurring or loss of vision called Uhthoff’s phenomenon.
The brain is usually quite good at compensating for the signals coming from the eyes at different speeds, but the one thing it is poor at doing is adjusting for depth perception. The reason we have two eyes with overlapping visual fields or binocular vision is for depth perception. This is why pwMS with previous optic neuritis may have poor depth perception, which affects their ability to judge where for example a cup or glass is on the table and as a result of this they often spill drinks. PwMS will also have difficulty playing ball sports such as tennis, table tennis or any sport that requires accurate depth perception.
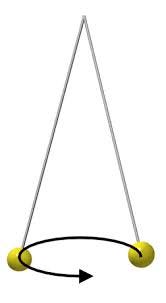
The delay in conduction between the abnormal nerve and the normal nerve can cause the brain to misinterpret visual inputs and result in abnormal or paradoxical depth perception. For example, a swinging pendulum is seen in 3D, with x, y and z (depth) dimensions when in reality it is only swinging in 2D (x, y). This is called the Pulfrich effect. The movie industry has hijacked this phenomenon. The glasses that are used to watch 3D movies filter light differentially between the two eyes, which then stimulate different populations of retinal photoreceptors. The retinal nerves transmit these different signals at slightly different speeds to the cortex, which the brain then perceives as being in 3D.
One function that seems to be very sensitive to this phenomenon is the judgment of distances whilst driving at night; for example, estimating how far you are from the traffic intersection or a stop sign. Many of my patients don’t like driving at night because of this. Why? Well, the brain uses a process called parallax to compensate for the loss of depth perception; i.e. the brain uses the relative size of familiar objects to help make a judgment on how far something is away from you in the distance. By using parallax somebody who is blind in one eye can judge depth and distance relatively well. However, at night in the dark when images are not well illuminated and the use of colour vision drops judgement by parallax fails and depth perception deteriorates.
I would be interested to know if any of you have any of these problems with depth perception and driving at night. If you do the chances are that you have had optic neuritis in the past.
Unfortunately, there is little we can do to treat this phenomenon, but knowing about and understanding why it occurs may help you compensate for this impairment, disability or handicap.

Parallax: Have you ever wondered why the setting sun and full moon on the horizon look so big compared to it being smaller when it is above us in the sky? It is actually not bigger; simply having a reference on the horizon (trees, mountains, buildings, the sea, etc.) makes your brain perceive it as being larger, i.e. closer. This is how parallax affects how the brain works and judges distance from you to an object in the distance.
Subscriptions and donations
Paid subscriptions to MS-Selfie are being used to administer the Newsletter and associated MS-Selfie microsite that is currently in development. At the request of several readers, I have now added the option of making a one-off donation. To keep this initiative open to all readers, I would appreciate it if those who can afford a subscription please subscribe. For active paying subscribers, thank you; your contribution is much appreciated.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry or Barts Health NHS Trust. The advice is intended as general advice and should not be interpreted as personal clinical advice. If you have problems please tell your own healthcare professional who will be able to help you.
Hello Doctor- (MS since 30, now 65, Betaseron 23 yrs). Optic neuritis was one of my early issues (3-6 years in). Two times one eye, one time the other. First two episodes clear onset and remissions 6-8 weeks, but the third episode was more gradual and 6 or more months with slower onset and remittance. I too had difficulty heading down on stairs (resolved now). Didn’t have problems with coffee cups etc. Driving at night was only in familiar places as tremor and nystagmus made it difficult to see things quickly (taking time for eyes to rest on objects in order to see them clearly, which when driving- you need this kind of instantly). I suppose judging distance at night would be difficult to compare before and after MS(?) unless it were strikingly obvious. (If the item is smaller, it must be farther away).
So depth is not an issue but it takes me a extra moment or two (depending on body temp) to settle my eyes on something to examine. Highway signs on a freeway in unfamiliar places leads to missed exits. I can see the same signs better at night. It’s best to examine road trips before you depart with a good map and count streets, etc. so you are prepared. And nystagmus makes having an easygoing optometrist not in a hurry important, when testing for a new glasses prescription!
{On a side note, I would be interested someday in interacting about 1) intermittent catheterization- Is it for health reasons or convenience?; and 2) differentiating between leg problems from MS and others which might come along anyway as you age (i.e. PTTD or Peroneal Neuropathy)}
J
Hi Professor.
We can fix this, this year in a measurable way by using cheap at home EEG devices.
This is my forth time now typing this as a comment, not sure what is wrong with this site, it likes to delete my comment.
Please get in touch to at least tell me why I am wrong.
Kind regards,
Benjamin Pettit.