
Tolebrutinib treatment algorithm 2.0
The aim of the diagram is to demonstrate how complex things become when you start to divide non-relapsing SPMS into subgroups.

The FDA’s decision not to license tolebrutinib for non-relapsing secondary progressive MS has activated the MS community. We have therefore written a commentary on the FDA’s position on tolebrutinib and want to include a diagram to demonstrate how complex treatment algorithms become when you start to subdivide the population eligible for treatment. If you are new to this issue, please read last week’s Q&A or listen to the accompanying podcast and catch up with yesterday’s newsletter and version 1.0 of the algorithm.
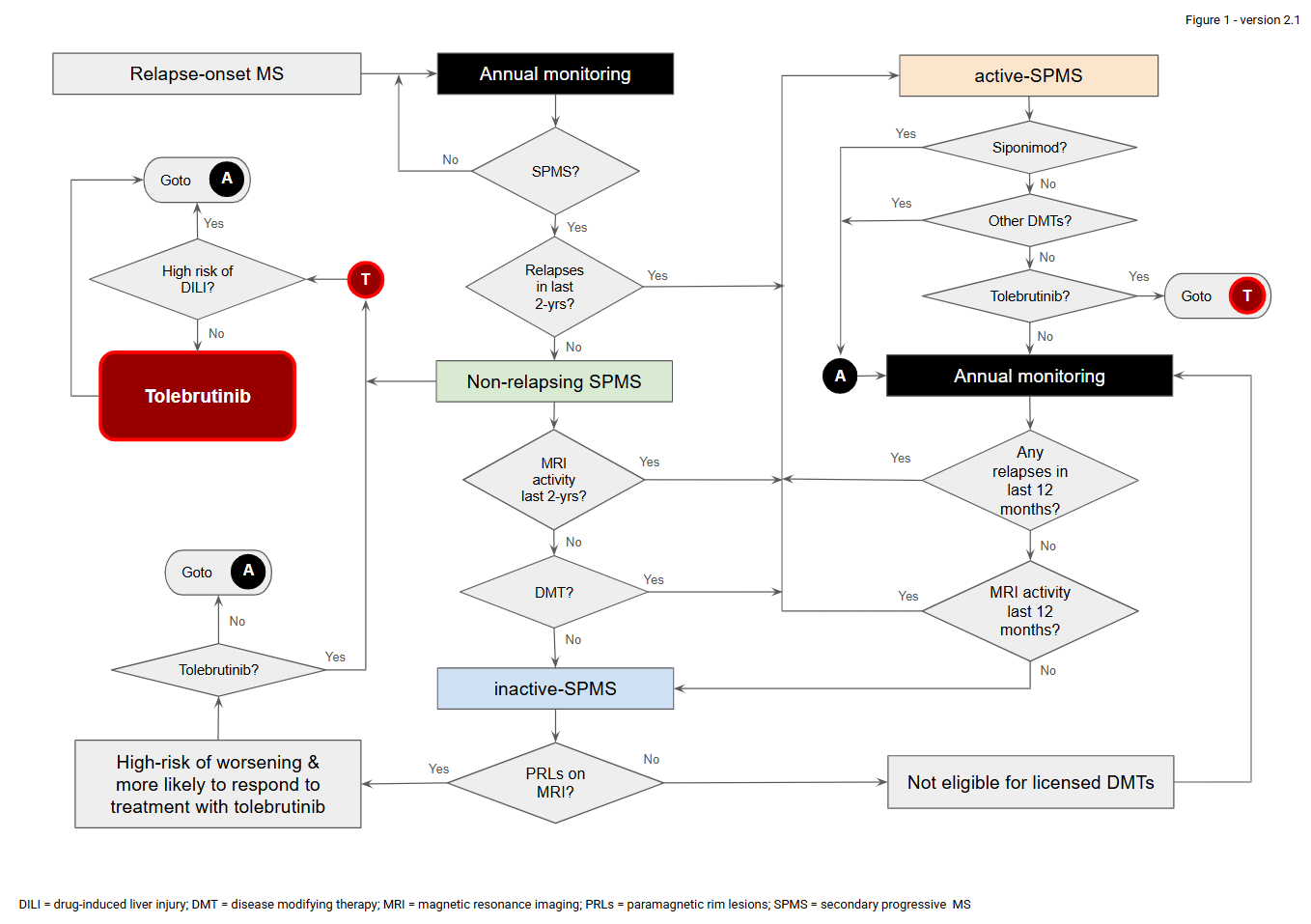
Figure legend
At present, a patient who is considered to have secondary progressive MS (SPMS) is classified as having non-relapsing MS if there is no history of relapses in the preceding two years. These are the patients who would be eligible for tolebrutinib using the inclusion criteria for the HERCULES phase 3 trial. However, the FDA believes the small subgroup of patients with baseline Gd-enhancing lesions (~13%) who responded better to tolebrutinib would benefit most. However, these patients would be classified as having active-SPMS and would therefore be eligible for siponimod and potentially other licensed MS disease-modifying therapies, depending on the approved label in different countries. Please note that, in most countries, patients with inactive-SPMS who are receiving a disease-modifying therapy (DMT) are classified as having active-SPMS on the premise that the current DMT is suppressing disease activity (relapses and/or focal MRI activity). As this definition is not universal, patients with worsening disability despite being treated with a DMT should be eligible for tolebrutinib. Similarly, patients with active SPMS who are unsuitable for spiponimod or other licensed DMTs should have the option of being treated with tolebrutinib, which also has anti-inflammatory properties, i.e. reduces relapse rates and MRI activity. This then leaves the subgroup of patients with inactive-SPMS not on a DMT, who would not be eligible for DMTs. With annual clinical and MRI monitoring, over 50% of these patients would be expected to become active and become eligible for siponimod and potentially other licensed MS disease-modifying therapies over a 2-3 year period. One proposal is to determine whether patients with inactive SPMS have paramagnetic rim lesions (PRLs) on MRI. Based on a post-hoc analysis of the phase 3 tolebrutinib studies, the subgroup with PRLs benefited most from tolebrutinib therapy. For pragmatic reasons, we would favour a simple treatment algorithm, i.e., based on the HERCULES inclusion criteria, which state that patients with non-relapsing SPMS are eligible for tolebrutinib treatment. Other pathways around this complex algorithm are potentially confusing and unnecessary if the DILI associated with tolebrutinib can be appropriately derisked.
I have tried to incorporate all your comments and positions. There are now no dead ends, and the algorithm allows for all eventualities.
The aim of the diagram is to demonstrate how complex things become when you start to divide non-relapsing SPMS into subgroups. A much simpler algorithm is to allow patients with non-relapsing SPMS access to tolebrutinib. After all, this is the population that was studied in the HERCULES trial.
Does version 2.0 make sense to you? If you have or may have SPMS, could you navigate the algorithm? We have to submit the figure for publication later this week. So there is still time for alterations.
Thanks.
Accidental readers
If you have been forwarded this email and are not an MS-Selfie subscriber, please consider subscribing and helping MS-Selfie expand its resources for the broader MS community. MS-Selfie relies on subscriptions to fund its curated MS-Selfie microsite, MS-Selfie books, MS-Selfie Infocards, and other activities that extend beyond the MS-Selfie Substack newsletters.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite and other related activities, as I don’t have time to do this myself. You must be a paying subscriber to ask questions unrelated to the newsletters or podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Questions
If you have questions unrelated to the newsletters or podcasts, please email them to ms-selfie@giovannoni.net. Prof. G will try to answer them as quickly as possible.
Important Links
🖋 Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have any problems, please tell your healthcare professional, who can help you.
Yes, this is much better; with those changes and clarity around the story you want to tell using it. At the end of the day, the Hercules criteria is simple and practicable. This also neatly exposes the Siponimod contradiction (logic flaw?).
The second figure is much more complex, but describes better the many variables...
I, sincerely, got to the point and understood better the first figure. Could you submit both on the report?
Since options, yes or no, are already present after each box, I don't think you need a question mark.