


Smouldering associated or SAW index and MS-CREATE a brain game
Could SAW have been detected earlier in these pwMS if cognition was being monitored using sensitive tests? Does it matter?

The majority of people with multiple sclerosis (pwMS) will have subtle worsening or smouldering-associated worsening (SAW) despite having no evident focal inflammatory disease activity (NEIDA). Clinical monitoring using validated outcome measures (EDSS, 9HPT, 25FTW, SDMT) is very insensitive at detecting SAW. This is particularly problematic early in the course of MS, where the impact of SAW is usually subclinical, i.e. not detected until a clinically apparent neurological deficit emerges gradually. I am sure many of you will relate to the slow creep of MS worsening and how you adapt to subtle changes in function before it hits you between the eyes. The latter typically happens when you try and do something strenuous that you haven’t done for some time, for example, attempting a long walk, or you have an infection and get temperature-related conduction block that exposes the deficits.
Another example many pwMS complain about is cognitive fatigue, which impacts their quality of life and occupational and social functioning. Approximately 50% of pwMS are unemployed ten years after their first symptoms of MS at a stage of their disease when they are not physically disabled. The cause of this unacceptably high rate of unemployment is almost undoubtedly cognitive dysfunction, cognitive and physical fatigue and other hidden symptoms of MS, in particular anxiety and depression. Could SAW have been detected earlier in these pwMS if cognition was being monitored using sensitive tests? Does it matter? It does, as identifying SAW allows one to potentially address it therapeutically.
Many different pathological processes within the central nervous system (CNS) are responsible for SAW that are potentially modifiable. Importantly, tolebrutinib, a CNS penetrant BTK inhibitor, which targets CNS resident B-cells and activated innate cells called microglia, has been shown to modify or slow down SAW independent of its relatively modest effects on focal inflammation (please see ‘ECTRIMS 2024 - battle of the BTKi's, 23-Sept-2024’, for more information on tolebrutinib).
Detecting SAW early may help identify pwMS eligible for tolebrutinib early on at a stage of their disease when they can derive the maximum benefit from tolebrutinib’s effects. Yes, when it comes to SAW, time is also brain; the earlier you target SAW, the better the long-term outcome for pwMS.
My colleagues and I are currently working on developing a SAW index. We envisage a new patient-reported outcome measure (PROM) specifically designed to detect SAW. Professor Jeremy Hobart, based at the University of Plymouth, is leading this project. If you want to volunteer to help develop the SAW index, please contact the study team via their website, Transform MS.

Another question is, can you modify SAW yourself with lifestyle modifications? I think yes, as many of the factors responsible for poor brain health may also make SAW worse. This is why I have been pushing for the holistic management of MS using the treatment philosophy of marginal gains, i.e., a slight improvement in many things that impact poor brain health, which, when added together, can make a big difference to MS outcomes.
We want to develop a cognitive game to help pwMS monitor and improve their cognition. The game must be addictive to engage pwMS in assessing their cognition and motivate them to improve their cognitive function. Firstly, do you think this is a good idea? And would you play such a game?
I play WORDLE and SPELLING BEE and do several other New York Times puzzles daily. I collect the results and share them via WhatsApp with my daughter, who also does them. This is a light-hearted family competition that allows us to check in with each other each day. Given my age, I am sure my daily routine is a form of cognitive prehabilitation or brain training. Can we make a game or a suite of mental games to stimulate you to train your brain and protect you from the effects of SAW while assessing your cognition? Suppose we can make the games competitive by using league tables or allowing you to share your results via social media. In that case, you can see how you are doing relative to others with MS and potentially people without MS. A core design philosophy is that this game needs to be as engaging to people without MS as it is for pwMS.
Cognitive Testing
The cognitive tests that are the best screen for cognitive dysfunction in MS tend to include a cognitive reaction time, i.e., you are given a mental task and then expected to react to it. The most widely studied and validated tests in MS include the PASAT (paced auditory addition test) and SDMT (symbol digit modalities test). The PASAT is probably superior because it has a learning effect and is the more cognitively strenuous and challenging of the two tests. As a result of this and the fact that pwMS find it stressful, the PASAT was sadly abandoned by the MS community and replaced with the SDMT.
We subsequently found that the learning effect of the PASAT test is a measure of cognitive reserve. In the fingolimod phase 3 studies, subjects who improved their PASAT scores at baseline, i.e., those who could learn, did much better than those who had no learning effect (see paper below). The learning effect predicted better disability outcomes regardless of whether trial subjects were on active treatment or placebo. In other words, the ability to learn a cognitive task and improve your performance is a measure of cognitive reserve or cognitive resilience. In short, the PASAT is a cognitive stress test. I have been pushing for the inclusion of cognitive stress tests into the assessment of MS for several years, but nothing has happened. I am not a neuropsychologist, so why would anyone listen to me? This may be the moment to make this happen. Do you agree?
Lessons from cardiology
When discussing neurological stress tests, I always use the analogy of the cardiologist assessing heart function. A cardiologist would never give you the all-clear from a cardiac perspective without doing a cardiac stress test. When I was a junior doctor (now called resident doctor) in general medicine, I spent many hours doing cardiac stress tests, i.e. making people walk and run on a treadmill whilst assessing their cardiac function symptomatically and with continuous ECG monitoring. In the late ‘80s, we used the Bruce and modified Bruce protocols to assess cardiac reserve. I think both these protocols have stood the test of time and are still being used today. The bottom line is that if you passed your cardiac stress test, i.e. had no evidence of ischaemic heart disease, you were discharged. If you failed your cardiac stress test, you had to have further investigations, typically a cardiac angiogram.
MS neurologists don’t perform neurological stress tests to detect SAW. We want to change this. Why?
We know that many pwMS who have EDSS 0, i.e. a normal neurological examination, have deficits when you look for them. Typical examples are cognitive dysfunction on formal psychometry, poor balance on a balance board, fatigue-related weakness on exercise, subtle hand incoordination when assessing fine finger movements, etc. I am aware that a minority of pwMS don’t want to know about these subtle deficits, but if detecting them has implications for how their MS is managed, their attitude may change; when I surveyed pwMS a few years ago for a talk I was doing at ECTRIMS on web-based self-monitoring, 12% of pwMS had what I called the ostrich syndrome—they simply didn’t want to know how MS was affecting their neurological functioning.
Why focus on cognition?
I don’t want the neurological stress tests to only focus on cognition; you have to start somewhere, and cognition is a logical place to start. Cognitive dysfunction occurs early in the course of MS, has an outsized inmpact on MS outcomes and impacts QoL and social and occupational functioning. In addition, it is the one domain in which loss of function scares pwMS. Another reason to focus on it is that it is often ignored in clinical practice because measuring it in clinical practice takes time, and time is one thing HCPs are short of.
Why gamify it?
I have been involved in many research initiatives using smartphone apps and wearables to measure neurological function. These apps and wearables achieve what they are meant to achieve, i.e., they measure neurological deficits in pwMS, but their adoption is dismally poor. PwMS download and use these apps but invariably stop using them after a few weeks. Why? Firstly, these apps are time-consuming; one project I was involved in required people to spend over an hour each week completing tasks. Time is precious even for pwMS wanting to monitor their MS.
Secondly, these apps tend to be boring; once you have completed the tasks and returned to the app for repeat measurements, you get the same old tasks. The tasks are static and don’t evolve by getting more challenging each time they are done. There is no learning to be done; we need to be able to assess learning effects to be able to determine reserve capacity. In short, these apps did not have built-in reward systems, which are essential to get pwMS to return to the app repeatedly. People play and get addicted to games because there is a natural tendency to want to improve and beat yourself and others by improving each time you play the game.
Thirdly, these apps are often poorly designed and simply not engaging. I can’t stress how important design is in making the experience of engaging with an application enjoyable. This is why I won’t design the game(s) myself. I intend to partner with some of the best designers in the field. Yes, this will cost money and go far beyond what MS-Selfie collects in subscriptions.
Finally, to the best of my knowledge, none of the MS monitoring apps have been socialised, i.e. to allow you to share or compare your current results with your previous ones and then share your results with others. Most of the most successful games work because they are competitive and allow between players comparisons. Let’s get competitive….
Cardboard and Lego 9-hole peg tests (c9HPT & Lego-9HPT)
When we designed and made an environmentally friendly cardboard 9HPT so that pwMS could assess their upper limb function, we had no idea how it would be used. Many of our patients do these 9HPTs religiously as part of their home monitoring routine. However, a few pwMS use their 9HPT to improve their upper limb function; they repurpose the 9HPT as a rehabilitation tool. I also developed the Lego-9HPT to encourage pwMS to construct a 9HPT out of Lego and just maybe play with their Lego sets. Playing Lego is a form of self-administered upper limb and hand rehabilitation, and if done in a group, it helps improve your social health. The idea of using Lego came from a survey we did of pwMS, asking them what they valued most about their upper limb function. An older man with MS answered that the most important thing to him was being able to play Lego with his grandchildren.
The idea of using the 9HPT as a rehabilitation tool upset some of my colleagues, who said this would disrupt clinical trial results. In other words, they didn’t want pwMS to do upper limb rehabilitation and improve their 9HPT scores, as it would affect their trial results. Their position is folly; what happened to the maxim ‘use it or lose it’? In response, we launched our ‘Under&Over’ project to nudge people with more advanced MS to do self-administered upper limb exercises at home. The Under&Over project got mixed results; maybe the exercise was not stimulating enough, competitive or addictive (see paper 2 below).
The Multiple Sclerosis Cognitive REAction Time gamE (MS-CREATE)
The first underlying principle is that MS-CREATE should be simple; simplicity has beauty, which is the charm of WORDLE and SPELLING BEE. This is where we need your help. Do you have any ideas that could be used for MS-CREATE? You may already play regular cognitive games to improve your brain health. If you do, what are they?
The following is an example of a potential game for MS-CREATE. The concept underpinning the game is from the SDMT. Sadly, there are very few original ideas regarding cognitive testing. The basic concept is to use shapes, symbols, and coloured objects to identify the stimulus from a range of objects. The idea would be to see how long it takes to get ten right; if you don’t get ten right in 60 seconds, you must start over again or accept that you have reached your ceiling. The stimulus would stay on the screen as a prompt on the game's lower levels; this would be less about memory.
MS-CREATE will need to get incrementally more challenging to find a ceiling. It is crucial to make the game difficult for even ordinary people. We need normal people to play the game to get an idea of the normal distribution of performance. A higher level of the game would involve having to rotate the object mentally to identify it from the list of choices. In other words, you must mentally manipulate the symbol to determine the matching image. The lower levels would have simple 2D shapes, but higher levels could include 3D shapes, adding complexity to the task. Don’t forget we want this game to be a stress test. The only way to create a stress test is to make the game increasingly difficult.
Once you have completed level one, you will be asked to remember the stimulus, i.e., there will be no prompt. It would then disappear before the range of choices became available. This test will involve memory and reaction times, and again, the memory test will become incrementally more difficult.
The point is to increase the game's difficulty so that you eventually reach a limit used to determine your score. Your scores will be logged, tracked over time, fed back to you, and logged on a leaderboard.
We also envisage using coloured symbols to add colour vision, another poorly monitored function in clinical practice, to the mix. The shades or colour contrast would become incrementally more complex, adding variation to the game.
Education
I never miss an opportunity to educate people about MS. Therefore, every time you play the game, the game will close by giving you a tidbit of information about MS and a link to an MS Selfie page that teaches you more about the relevant topic.
For example: “Did you know that pwMS who have hot microglia detected using PET (positron emission tomography) are more likely to have SAW (smouldering MS associated worsening)?”
Click here for more information on hot microglia and SAW.
The idea of using CREATE-MS for education comes from an app I used to subscribe to called CURIOSITY (for curious minds). It provided a daily fact and a back story to that fact. Sadly, CURIOSITY was acquired by the Discovery Channel and shut down.
Why a game and not an outcome measure?
If we did MS-CREATE as an outcome measure, we would need to design a formal proposal, define it as a medical device, get MHRA approval, etc. It is only worth going that route if the game works, i.e., it becomes engaging and addictive, and pwMS use it repeatedly. In addition, we would want it to go viral and get tens of thousands of pwMS playing it regularly. At this stage, if the game looks like it measures cognitive impairment and cognitive reserve and acts as a cognitive rehabilitation tool, we can then study it formally as an outcome measure. Another thing with medical devices and outcome measures is that regulatory agencies want them to be static, i.e. they approve a version. Then, it can’t evolve. Any new version has to be validated, etc. The latter is why CREATE-MS has to be, at first, a game and not an outcome measure.
Funding
We were planning to design this game as an independent project. However, with the added educational component, I think it should be included within MS-Selfie as a tool to help pwMS self-manage their MS. Do you agree? Do you have any ideas about funding? I suspect this project is going to cost a lot.
Disclaimer
Sanofi is funding the development and study of the SAW Index. Members of the SAW Index steering committee include Jennifer Graves, Fred Lublin, Gavin Giovannoni, Jiwon Oh, Tjalf Ziemssen, Joep Killestein, Melinda Magyari, Jose Manuel Garcia Dominguez, and Lukas Cepek.
Paper 1 - PASAT & LEARNING
Objective: To assess the prognostic value of practice effect on Paced Auditory Serial Addition Test (PASAT) in multiple sclerosis.
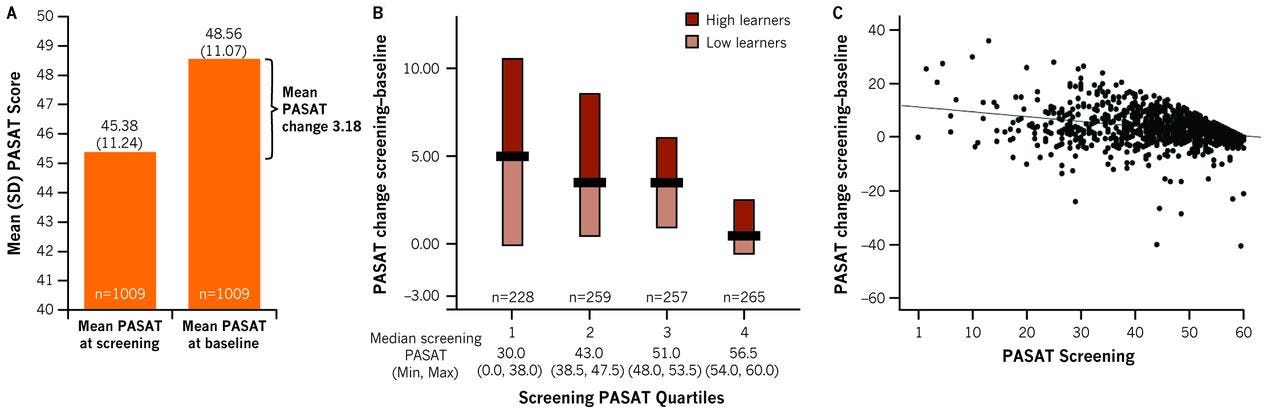
Methods: We compared screening (day -14) and baseline (day 0) PASAT scores of 1009 patients from the FTY720 Research Evaluating Effects of Daily Oral therapy in Multiple Sclerosis (FREEDOMS) trial. We grouped patients into high and low learners if their PASAT score change was above or below the median change in their screening PASAT quartile group. We used Wilcoxon test to compare baseline disease characteristics between high and low learners, and multiple regression models to assess the respective impact of learning ability, baseline normalised brain volume and treatment on brain volume loss and 6-month confirmed disability progression over 2 years.
Results: The mean PASAT score at screening was 45.38, increasing on average by 3.18 from day -14 to day 0. High learners were younger (p=0.003), had lower Expanded Disability Status Scale score (p=0.031), higher brain volume (p<0.001) and lower T2 lesion volume (p=0.009) at baseline. Learning status was not significantly associated with disability progression (HR=0.953, p=0.779), when adjusting for baseline normalised brain volume, screening PASAT score and treatment arm. However, the effect of fingolimod on disability progression was more pronounced in high learners (HR=0.396, p<0.001) than in low learners (HR=0.798, p=0.351; p for interaction=0.05). Brain volume loss at month 24 tended to be higher in low learners (0.17%, p=0.058), after adjusting for the same covariates.
Conclusions: Short-term practice effects on PASAT are related to brain volume, disease severity and age and have clinically meaningful prognostic implications. High learners benefited more from fingolimod treatment.
Paper 2 - Under&Over
Background: Impairment of upper limb function is common in Multiple Sclerosis (MS). Rehabilitation remains a key strategy to manage symptoms and improve quality of life. The Under & Over study assessed the effectiveness of a rehabilitation programme in people with advanced MS.
Objective: To determine if repeated use of Under & Over can improve upper limb function for people with MS.
Methods: One hundred and six (N = 106) people with MS participated in this 3-month study. The primary outcome measure was the cardboard 9-hole peg test (c9HPT), with secondary outcomes including the EuroQol-5Dimensions, 5-Level Questionnaire (EQ5D-5 L) questionnaire. There were three arms: Arm 1a, the 'Daily Group', engaged with the Under & Over tool daily for 30 min. Arm 1b, the 'Free Use Group', used the same tool without time constraints, with the added feature of a community sharing platform. Arm 2, the 'Delayed Start Group', initially completed the c9HPT for three months before switching to the 'Free Use' programme.
Results: 43/106 (41 %) of those randomised completed the primary end point. No significant difference between c9HPT at baseline and 3 months was seen in Arm 1a or 1b. Participants in Arm 2 who had been completing the c9HPT 5 days a week for 3 months showed a training effect in the dominant hand (mean speed at baseline 0.0455 (s-1), mean at 3 months 0.0341, difference 0.011; 95 % CI 0.0080 to 0.0148, p < 0.001). No significant difference was seen in c9HPT time following 3 months of active use of the Under & Over tool. The study faced significant limitations, notably in participant adherence, with fewer than half (43/106 (41 %)) completing the final assessment.
Conclusions: This study demonstrates how a small, engaged, and motivated group were able to complete a remote rehabilitation programme. Future remote intervention studies could benefit from incorporating adaptive engagement strategies, such as personalised reminders and participant-tailored activity adjustments, to enhance adherence and capture a broader spectrum of patient experiences.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. You must be a paying subscriber if people want to ask questions unrelated to the Newsletters or Podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
X (Twitter) / LinkedIn / Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.
Email reply:
I hope you are keeping well. Just read the MS Selfie about games, very interesting. I too am sorry the PASAT test has been stopped
I do Sudoku from the Times. Only on mild level and I admit I make mistakes and can check for errors. If I get stuck then I will cheat. I enjoy Tuesday, Thursday and Friday when the puzzle I like is published. I believe it helps to keep my brain active but I must stop cheating. Each game takes me about 30 - 45 minutes. I must also restart playing backgammon on my laptop but need to find a new version.
I also get outdoors to do the shopping and cook the evening meal. Cooking involves lots of motor and memory skills such as have I salted the water, reading the recipe, chopping the vegetables etc and I enjoy it. When our kitchen is redone I'm going to restart cake baking. It is another activity that, I think, requires many motor and memory skills.
My wife and I play a board game each week. Our skill levels are compatible, once again requires concentration and motor skills. We both Carcasonne and Ticket to Ride and also play a few others. I also want to start playing bridge again, had to stop in the pandemic. I'm not very good but once again you need memory, concentration and social skills. It is competitive but a safe space at the same time.
Just a few ideas that might help other people. I must get out for a walk using my walker, its very important to get the exercise and fresh air. No shopping for me today.
Surely what MSers really need are treatments which effectively address SAW, and minimise the CNS tissue damage and unrelenting disability progression. Rather than creating games, why not put effort into fast tracking tolebrutinib? We keep being told that time is brain and that SAW / PIRA are the main causes of CNS tissue destruction, but I’d hazard a guess that tolebrutinib won’t be available from another 2 years (with criteria which will limit access). As we near 2025, I do wonder what MS researchers have been up to for the last 50 years given that for the vast majority of MSers disability progression continues regardless of the treatment chosen. My friends recently diagnosed with cancer (breast, prostate) have a completely different treatment experience - no Lego or designing games, and no self- management. The treatment target is to get them cancer free and back to good health. Neurology patients can only dream of this.