


Rising incidence of MS in women: what is the telling us about the cause of MS?
I don’t have the answer to this MS mystery. If any of you have any ideas, please let me know.

If EBV is the cause of MS, how can we explain the changing sex ratio of the disease?
To prove that MS is caused by a single factor or the interaction of several factors, we must explain everything we know about the disease's epidemiology. If EBV is the cause of MS, how does EBV explain why relapsing-remitting MS (RRMS) is becoming more common in women? In comparison, the incidence of primary progressive MS (PPMS) remains constant, with an equal number of men and women affected.

Please note that the change in sex ratio is not universal; for example, it has not been noted in Sweden. Another outlier here is Iran, where the sex ratio of F:M was very high and has subsequently come down. In 2006, the F:M sex ratio was 3:1, which is very high, and it has since decreased to 2.2:1 in 2017. The ratio ascended from 2006 to 2010, increasing from 3.1 to a peak of 3.5, respectively, and a descending pattern from 2010 to 2017, decreasing from 3.5 to 2.2.
Some commentators suggest the changing sex ratio is due to the change in smoking prevalence amongst women, which has been increasing relative to males since the end of the Second World War. However, Iran is also an outlier here as less than 10% of Iranian women smoke compared to more than 30% of Iranian men. I am, therefore, unconvinced that smoking explains the changing sex ratio of MS incidence and why is the sex ratio of pwPPMS not changed?
Some blame cultural factors, such as the addition of UV blockers in cosmetics over the last twenty-plus years and other cultural changes that have caused women to shun sun exposure, resulting in women more likely to become vitamin D deficient.
Others have suggested the use of oral contraceptive pills (OCP) or a change in the work environment. However, the change in sex ratio appears to go back to the beginning of the 20th century, so it predates the change in the work environment associated with World War II or the introduction of the OCP in the ’60s.
The changing sex ratio, or lack of change in some regions, or the dynamic changes in countries such as Iran tell us that it must be driven by environmental factors and, hence, reversible. The changing sex ratio has also been used as a proxy for a rising incidence of MS.
I don’t have the answer to this MS mystery. If any of you have any ideas, please let me know. What I do know is that MS is much more common in women, and hence, it could badged as a pink-ribbon disease.
Relevant papers
BACKGROUND: Incidence of multiple sclerosis is thought to be increasing, but this notion has been difficult to substantiate. In a longitudinal population-based dataset of patients with multiple sclerosis obtained over more than three decades, we did not show a difference in time to diagnosis by sex. We reasoned that if a sex-specific change in incidence was occurring, the female to male sex ratio would serve as a surrogate of incidence change.
METHODS: Since environmental risk factors seem to act early in life, we calculated sex ratios by birth year in 27 074 Canadian patients with multiple sclerosis identified as part of a longitudinal population-based dataset.
FINDINGS: The female to male sex ratio by year of birth has been increasing for at least 50 years and now exceeds 3.2:1 in Canada. Year of birth was a significant predictor for sex ratio (p<0.0001, chi(2)=124.4; rank correlation r=0.84).
INTERPRETATION: The substantial increase in the female to male sex ratio in Canada seems to result from a disproportional increase in the incidence of multiple sclerosis in women. This rapid change must have environmental origins even if it is associated with a gene-environment interaction, and implies that a large proportion of multiple sclerosis cases may be preventable in situ. Although the reasons why the incidence of the disease is increasing are unknown, there are major implications for health-care provision because the lifetime costs of multiple sclerosis exceed pound1 million per case in the UK

Amongst 11152 multiple sclerosis patients who were evaluated from 2006 to 2017, there was a significant reduction (P-value=0.01) in female to male ratio over the time from 3:1 in 2006 into 2.2:1 in 2017. This ratio changes demonstrated an ascending pattern from 2006 to 2010 (3.1 to 3.5, respectively), and also a descending pattern from 2010 to 2017 (3.5 to 2.2, respectively). Consequently there were significant changes in the female to male ratio by passing the time, with respect to the Pearson correlation coefficient (Pearson=−0.69, P=0.01).
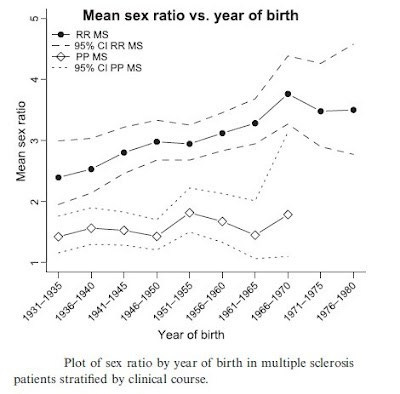
BACKGROUND AND PURPOSE: In a longitudinal population-based dataset of patients with multiple sclerosis (MS), we have previously observed a substantial increase in the female to male sex ratio in Canada over the last 50 years. Here, we aimed to determine whether this change in sex ratio is related to the clinical course of MS.
METHODS: We calculated sex ratios by birth year in 11 868 patients with relapsing-remitting (RR) MS and 2825 patients with primary progressive (PP) MS identified as part of the Canadian Collaborative Project on the Genetic Susceptibility to MS.
RESULTS: Year of birth was a significant predictor for sex ratio in RR MS (P < 0.0001, chi(2) = 21.2; Spearman’s rank correlation r = 0.67), but not for PP MS (P = 0.44, chi(2) = 0.6; Spearman’s rank correlation r = 0.11).
CONCLUSIONS: An increase in the number of female RR MS patients over time accounts for the increasing sex ratio of MS.
A remarkable increase in female to male ratio of multiple sclerosis (MS) is recognised in high incidence areas. Norway is a high-risk area for MS, spanning latitudes 58-71°N. We studied whether the sex ratio has changed over time and whether it differs by clinical phenotype or by latitude. Population-based epidemiological data and data from the Norwegian MS Registry on patients born from 1930 to 1979 were combined in this study. Place of birth was retrieved from the Norwegian Population Registry and information on clinical subtypes was obtained from the Norwegian MS Registry. The female to male ratio ranged from 1.7 to 2.7 (median 2.0) in 5,469 patients born in Norway and increased slightly by 5-year blocks of year of birth (p = 0.043). The sex ratio was 2.6:1 in 825 patients born 1970-1979, which is significantly higher than in those born 1930-1969 (p < 0.001). In patients with relapsing-remitting onset, the sex ratio was 2.4:1, while it was 1.1:1 in those with primary progressive disease. The sex ratio did not differ between the south, the middle and the north of the country. The overall sex ratio of MS is strongly determined by cases with relapsing-remitting onset. We did not observe the remarkable increase in sex ratios of MS reported from other high-risk areas. The high sex ratio in the youngest birth cohorts may change as an increasing proportion of cases in this age group is being diagnosed. Sex ratio was not associated with latitude.
Background: Sex ratio in multiple sclerosis has been reported from several geographical areas. The disease is more common in women. In Europe, the female-to-male ratio varies from 1.1 to 3.4. A recent study from Canada has reported a significant increase, with time, in female-to-male ratio in multiple sclerosis over the last 100 years.
Objective: The aim of this study was to analyse any change in sex ratio in multiple sclerosis in the Swedish population.
Methods: Data from the Swedish MS Register and data from the Swedish National Statistics Office were used to estimate sex ratio by year of birth and year of onset.
Results: In the analysis of sex ratio by year of birth there were 8834 patients (6271 women and 2563 men) born between 1931 and 1985. The mean women-to-men ratio was 2.62. No clear trend was noted for the women-to-men ratio by year of birth (Spearman’s rho = 0.345, p = 0.298, n = 11). The number of patients analysed by year of onset was 9098 during the time period 1946 until 2005. The mean women-to-men ratio was 2.57. No significant change in women-to-men ratio (Spearman’s rho = -0.007, p = 0.983, n = 12) with time was observed.
Conclusion: There is no evidence for an increasing women-to-men ratio with time amongst Swedish multiple sclerosis patients.
BACKGROUND: A female/male (F/M) ratio increase over time in multiple sclerosis (MS) patients was demonstrated in many countries around the world. So far, a direct comparison of sex ratio time-trends among MS populations from different geographical areas was not carried out.
OBJECTIVE: In this paper we assessed and compared sex ratio trends, over a 60-year span, in MS populations belonging to different latitudinal areas.
METHODS: Data of a cohort of 15,996 (F = 11,290; M = 4,706) definite MS with birth years ranging from 1930 to 1989 were extracted from the international MSBase registry and the New Zealand MS database. Gender ratios were calculated by six decades based on year of birth and were adjusted for the F/M born-alive ratio derived from the respective national registries of births.
RESULTS: Adjusted sex ratios showed a significant increase from the first to the last decade in the whole MS sample (from 2.35 to 2.73; p = 0.03) and in the subgroups belonging to the areas between 83° N and 45° N (from 1.93 to 4.55; p<0.0001) and between 45° N to 35° N (from 1.46 to 2.30; p<0.05) latitude, while a sex ratio stability over time was found in the subgroup from areas between 12° S and 55° S latitude. The sex ratio increase mainly affected relapsing-remitting (RR) MS.
CONCLUSIONS: Our results confirm a general sex ratio increase over time in RRMS and also demonstrate a latitudinal gradient of this increase. These findings add useful information for planning case-control studies aimed to explore sex-related factors responsible for MS development.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. You must be a paying subscriber if people want to ask questions unrelated to the Newsletters or Podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
🖋 Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.
I think it was in interview with Gabor Mate I heard, in which he hypothesized that women have more autoimmune disease than men because of a multitude of factors that lead to increased cortisol levels. These included putting others needs above your own, caretaking in general, increased daily responsibility, etc. Regardless of the specific cultural/lifestyle contributions, I am intrigued about the role of cortisol in the development of these autoimmune diseases.
Is it anecdotal that more women are diagnosed soon after pregnancy? Pregnancy suppresses symptoms which return ( often significantly) afterwards which would suggest hormonal involvement? Women are more susceptible to auto immune conditions which are being more frequently recognised?