

I am sure many of you won’t want to know about the underbelly of living with advanced MS. As pwMS become more disabled, complications of being immobilised start to appear. The one that worries all HCPs working with patients who have MS is pressure sores or ulcers.
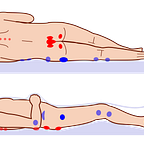
Pressure ulcers remain a devastating clinical challenge encountered in the management of people with advanced MS. Pressure ulcers, pressure sores, bedsores, decubitus ulcers, or pressure injuries, are localised areas of cellular necrosis and tissue damage occurring in the skin and underlying soft tissues. They almost exclusively develop over bony prominences such as the sacrum, ischial tuberosities (hips), heels, and occiput (back of head). The following image from Wikipedia illustrates the most common sites for pressure ulcers.

MS does not intrinsically or directly cause skin breakdown; however, motor and sensory loss, autonomic dysfunction, spasticity, and cognitive impairment associated with advanced MS are risk factors for pressure sores.
The economic burden of pressure sores is very high and continues to escalate globally. In the UK, pressure ulcers rank among the top 10 harms in the NHS, affecting hundreds of thousands of patients annually. In 2004, pressure ulcers were estimated to cost the NHS between £1.4 billion and £2.4 billion per year, representing approximately 4% of total NHS expenditure at the time. More recent estimates indicate that the management of pressure ulcers costs the NHS over £3.8 million every single day. At an individual level, pressure ulcers diminish a patient’s health-related quality of life. The condition frequently confines individuals to strict bed rest, exacerbates social isolation, causes pain, and introduces the risk of life-threatening complications such as osteomyelitis and septicemia.
I recall when I was a very junior neurology trainee looking after a young woman with MS and a large cavitation pressure ulcer over her sacrum. She spent more than 6 months on the ward having the pressure sore managed. Sadly, shortly after discharge, she developed recurrent septicaemia and passed away from infection. Whenever I see a patient with a pressure sore, I have flashbacks to my experience with this patient.
The management of pressure ulcers within the MS population is complex and requires a multidisciplinary team to manage spasticity, pain and frequently immobility. Care pathways have shifted away from reactive wound care toward highly proactive, multidisciplinary prevention strategies integrated within frameworks like the National Wound Care Strategy Programme (NWCSP). The intersection of clinical care, patient safety, and legal accountability in the UK has transformed the reporting and management of severe pressure ulcers. Regulatory bodies, such as the Care Quality Commission (CQC), alongside legislative frameworks such as the Care Act 2014, have established notification and safeguarding protocols. These legal mechanisms are designed to determine whether severe tissue damage represents an unavoidable consequence of terminal clinical decline or a physical manifestation of systemic neglect and institutional failure. Yes, pressure sores are a notifiable condition under the NHS and must be investigated.
Mechanisms of tissue failure
The aetiology of pressure ulcers in pwMS is multifactorial. The injury involves prolonged mechanical loading on soft tissues compressed between an external support surface—such as a mattress, wheelchair seat, or orthotic device—and an internal skeletal structure. The continuous pressure, friction, and shear forces are responsible for tissue injury. Under normal conditions, capillary closure pressure is approximately 32 mmHg. When external mechanical pressure exceeds this threshold for a sustained period, localised tissue perfusion is severely compromised. This results in hypoxia, the accumulation of metabolic waste products, and subsequent cellular necrosis. Vulnerable individuals lacking the capacity for spontaneous movement, irreversible ischaemic damage can commence in as little as 20 minutes.
Shear forces represent a particularly insidious and destructive mechanism. Shearing occurs when the epidermal layer remains stationary against a support surface, anchored by friction, while the underlying skeletal structures and deep fascial layers shift or slide. This dynamic is frequently observed when a patient with poor core control slides down the incline of a hospital bed or assumes a slumped posture within a wheelchair. This parallel, opposing force severely distorts, stretches, and ultimately ruptures deep fascial blood vessels, initiating ischaemia from the deep muscle tissues outward toward the skin. This mechanism frequently results in suspected deep tissue injuries that cause massive subdermal necrosis while initially presenting only as intact, discoloured skin on the epidermal surface. Friction, conversely, acts directly on the epidermal layer. Functioning like sandpaper, friction physically strips away the protective stratum corneum during transfers or spasms, drastically lowering the tissue’s threshold for pressure-induced necrosis and exposing deeper layers to bacterial colonisation.
While these mechanical forces are the direct forerunners of ulceration, the intrinsic neurological deficits imposed by MS render the tissues susceptible to injury, stripping away the body’s natural defensive mechanisms. Advanced MS is usually associated with paraparesis or quadriparesis, which is associated with a lack of spontaneous micro-movements and weight-shifting behaviours that healthy individuals continuously utilise to redistribute weight and permit capillary reperfusion during sitting or sleeping. At the same time, damage to the ascending sensory pathways results in significant hypoaesthesia or complete anaesthesia. The loss of protective pain feedback, which would normally alert the brain to impending tissue ischaemia and a change in posture, is reduced or lost in advanced MS.
Spasticity (hypertonia), muscle spasms, and joint contractures alter resting posture, often forcing limbs into unnatural and asymmetrical positions, and create friction and shear forces as the patient’s body rubs against support surfaces during movement of spasms.
Comorbid bladder and bowel dysfunction leads to frequent urinary and faecal incontinence. Prolonged exposure to moisture, along with bacterial and fungal overgrowth, macerates the epidermis. Moisture accelerates frictional damage and introduces the complicating factor of moisture-associated skin damage (MASD), which frequently co-occurs with pressure ulceration.
Advanced MS is often accompanied by dysphagia, fatigue, and severe depression, all of which contribute to reduced caloric and protein intake. This leads to malnutrition and low albumin levels. Skin integrity is intrinsically linked to nutritional status; malnourished, hypoalbuminaemic tissues lack the amino acid substrates required for repair, collagen synthesis, and maintenance of interstitial oncotic pressure, resulting in oedema and diminished resistance to hypoxic stress.
Epidemiology
Pressure ulcers are a pervasive, escalating global health crisis, exacerbated by ageing populations, increasingly fragmented care networks, and the rising prevalence of complex chronic diseases. In the Global Burden of Disease (GBD) Study, report that the incident cases of pressure ulcers more than doubled from 1,142,594.8 in 1990 to 2,468,317.5 in 2021, and the resultant mortality attributed to pressure ulcers rose from 16,741.1 to 37,032.7 globally, and DALYs surged from 408,887.0 to 803,747.4 over the same period.
Despite these increases in absolute burden driven by population growth and ageing, the age-standardised incidence rate (ASIR) decreased slightly, indicating that, while the total number of patients suffering is higher, the per-capita risk, when adjusted for age, has stabilised or marginally improved due to preventive measures.
Sadly, the burden of pressure ulcers correlates with the socio-demographic index (SDI), with significantly higher burdens observed in elderly females and a rising incidence in elderly males.
In a prospective cohort study of 185 pwMS without existing skin breakdown, the incidence rate of developing a new pressure ulcer was documented at 10.8% (20 patients) (see paper below). The development of pressure ulcers was not random; predictors of tissue failure included a history of previous stroke, being bed- or chair-bound, poor nutrition and urinary or faecal incontinence.
In the UK, pressure ulcer prevalence in highly dependent populations ranges from 11 to 13%. However, when looking strictly at wheelchair users—who constitute a large and vulnerable proportion of patients with advanced MS—registry studies indicate varying prevalence rates heavily dependent on the underlying neurological pathology. Among young wheelchair users overall, 55% experience at least one pressure ulcer a decade post-injury or disease onset. Specifically within the MS sub-population of chronic wheelchair users, the cross-sectional prevalence of current pressure ulcers is estimated at 4%.
Within intensive care units (ICUs) and orthopaedic surgical wards where MS patients may be admitted during severe disease relapses or for unrelated acute pathologies, incidence rates peak dramatically. General ICU prevalence averages 6.8%, with an incidence rate of 3.8%. Orthopaedic surgery wards have alarmingly high incidence rates of 18.5%, emphasising the danger of prolonged surgical immobilisation.
The sacrum is overwhelmingly the most affected area, accounting for up to 68% of ulcers, followed closely by the heels, left and right trochanters, and ankles. When analysing severity across generalised hospital populations, stage 1 and stage 2 ulcers account for the vast majority (45% each), while severe stage 3 and stage 4 ulcers occur at 4% each.
Clinical classification and staging systems
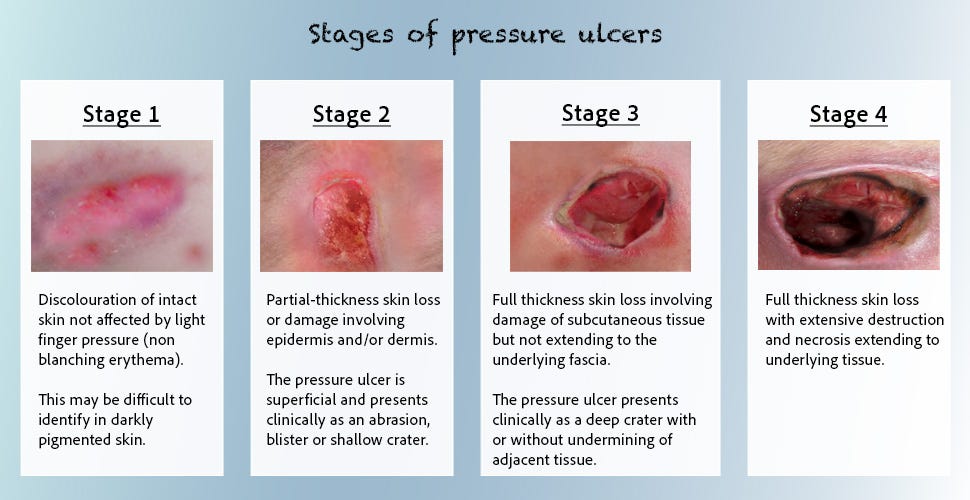
The management and reporting of pressure ulcers in the UK rely on internationally validated classification frameworks. The clinical staging system is based on the depth of visible tissue destruction:
Stage 1: Non-blanchable erythema of intact skin. The skin remains unbroken, but localised discolouration, warmth, oedema, or induration is present. In darkly pigmented skin, this may appear as a distinct alteration in colour or tissue consistency rather than classic redness.
Stage 2: Partial-thickness skin loss involving the epidermis, dermis, or both. This presents clinically as a shallow, open ulcer with a red-pink wound bed, devoid of slough, or as an intact or ruptured serum-filled blister.
Stage 3: Full-thickness skin loss involving damage to or necrosis of subcutaneous fat. Bone, tendon, and muscle are not exposed. Slough may be present, but it does not obscure the depth of tissue loss. Undermining and tunnelling may occur.
Stage 4: Extensive, full-thickness tissue loss with exposed or directly palpable bone, cartilage, tendon, or muscle. Slough or eschar may be present on some parts of the wound bed, and osteomyelitis is a frequent complication.
Unstageable: Full-thickness tissue loss in which the base of the ulcer is completely covered by slough (yellow, tan, grey, green, or brown) or eschar (tan, brown, or black) in the wound bed. The true depth cannot be determined until the eschar is surgically or autolytically debrided.
Suspected deep tissue injury (DTI): A purple or maroon localised area of discoloured intact skin or a blood-filled blister due to damage of underlying soft tissue from pressure and shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, or warmer or cooler than adjacent tissue. These injuries can progress rapidly, exposing additional layers of tissue, even with optimal treatment.
Screening and risk stratification protocols
Given the rapid onset of ischaemic tissue damage—and the consequences of progression—rigorous, routine screening protocols are important. The National Institute for Health and Care Excellence (NICE) provides guidelines (specifically NG220 for Multiple Sclerosis and CG179 for Pressure Ulcers) mandating aggressive risk assessment and proactive intervention for adults living with MS.
NICE guideline NG220 explicitly dictates that healthcare providers must check patients with MS who have severely reduced mobility at every single clinical contact for areas at risk of pressure ulcers. Furthermore, any person with MS who utilises a wheelchair requires a formal clinical assessment specifically targeting pressure ulcer risk. This assessment must lead to the development and documentation of a personalised risk minimisation action plan, and the individual must be thoroughly informed of their risk status. Whenever a patient with MS is admitted to a hospital, secondary care facility, or tertiary care environment—regardless of the primary reason for their admission—their immediate need for pressure-relieving devices and procedures must be evaluated.
Comprehensive screening goes beyond mere skin examination. The baseline assessment tools linked to NICE NG220 demand a holistic review utilising functional scales that quantify the total level of disability, such as the EDSS, the MSFC, the Cambridge MS basic score (CAMBS), or the functional assessment of MS (FAMS). Clinicians must also assess for factors that worsen spasticity, evaluate cognitive functions that might impair a patient’s ability to self-monitor, and review personal and social care needs, including the availability of community caregivers.
Limitations of standardised scales
In general clinical practice, standardised risk assessment tools such as the Norton Scale, Waterlow Scoring System, and the Braden Scale are utilised to quantify a patient’s vulnerability. These instruments aggregate sub-scores across domains, including sensory perception, skin moisture, physical activity, mobility, nutritional status, and friction and shear. However, clinical evidence and UK consensus guidelines caution against relying solely on these numeric scores for patients with MS. These standardised scales were primarily validated in geriatric populations and place heavy weight on chronological age. Consequently, a younger patient in their thirties or forties with advanced SPMS might automatically score as “low risk” due to their youth, despite possessing profound paraplegia, severe unrelenting spasticity, and complete pelvic sensory loss. Furthermore, tools such as the Waterlow score often omit or inadequately quantify the violent, repetitive shear forces generated by neurogenic spasms. Therefore, UK clinical guidelines expressly state that the assessment must be a holistic clinical evaluation that specifically takes into account the unique features of MS, rather than simply recording and relying on a generalised pressure ulcer risk score.
Education and self-monitoring
Secondary prevention through patient self-monitoring is important. Teaching pwMS or their caregivers to perform rigorous daily visual and tactile skin inspections is critical. Patients are instructed to routinely check pressure points—heels, knees, hips, buttocks, and elbows—for the primary clinical marker of impending tissue necrosis: non-blanchable erythema. They should be taught that reddened areas of skin over bony prominences should fade within minutes after pressure is removed; if the redness does not dissipate, irreversible ischemic injury may have commenced, requiring immediate intervention by a district nurse. Specific diagnostic screening questions used by community nurses and caregivers assess for sudden changes in mobility, reductions in fluid or caloric intake, recent acute illnesses (such as influenza), significant weight fluctuations, and critical changes in the level of muscle spasms, which often serve as an early warning sign of impending skin breakdown.
Prevention and management
The management of pressure ulcers in MS necessitates a coordinated, multidisciplinary team approach. Because the variables contributing to ulceration cross multiple physiological systems, isolated nursing care is insufficient. Effective management comprises MS specialist nurses, tissue viability nurses (TVNs), general practitioners, neurophysiotherapists, occupational therapists, dietitians, and dedicated wheelchair/seating specialists. The national wound care strategy programme (NWCSP) outlines clinical pathways requiring early risk identification to ensure rapid access to these varied specialities, optimising individual outcomes and preventing the costs associated with worsening pressure sore severity.
Pressure ulcers cannot heal, regardless of topical interventions or surgical reconstruction, if the inciting physical forces remain present. It is therefore changing your posture. For seated patients with upper-body mobility, shifting weight slightly—such as rolling from cheek to cheek—every 20 minutes is strongly recommended to facilitate vital capillary reperfusion. Immobile patients confined to bed require strict turning schedules, traditionally executed every two hours, meticulously alternating between lateral, supine, and prone positions to redistribute mechanical load.
Occupational therapists and tissue viability nurses can prescribe pressure-relieving equipment. This includes alternating pressure air mattresses, profiling beds, and customised gel-filled or customised moulded wheelchair cushions that expand the surface area over which the patient’s weight is distributed. The use of traditional “ring” or “doughnut” cushions is not recommended as they create a tourniquet effect, concentrating mechanical pressure on the surrounding tissues, occluding blood vessels, and paradoxically causing the exact pressure damage they are intended to prevent.
Neurophysiotherapists will teach formal and informal caregivers how to transfer patients safely and, if necessary, how to use mechanical hoists, slide sheets, and transfer boards. Poor transfer techniques—such as manually dragging a patient across a bed—generate extreme friction and shear forces that rapidly strip the epidermal barrier and rupture deep vessels.
Wound healing is a catabolic process demanding energy, amino acids, and micronutrients. Dietitians frequently prescribe high-protein supplements, zinc, and vitamin C to bolster collagen synthesis and immune function. Clinical vigilance is especially required during acute infections, influenza, or MS relapses, as the basal metabolic rate increases, often accompanied by frequent drops in appetite, which elevates the risk of rapid skin failure.
Active wound care
When a pressure ulcer develops despite preventative measures, treatment algorithms escalate concurrently with the stage of the ulcer:
Conservative management: For stage 1 and 2 ulcers, the clinical focus relies on offloading, optimising the wound microenvironment using advanced dressings (hydrocolloids, alginates, or foams), managing incontinence to prevent MASD, and preventing secondary bacterial colonisation.
Advanced therapeutic modalities: For complex, highly exudative stage 3 and 4 wounds, negative-pressure wound therapy (NPWT) is frequently used. NPWT applies controlled sub-atmospheric pressure to the wound bed via a sealed vacuum system. This continuously extracts infectious exudate, reduces localised interstitial oedema, physically draws the wound edges together, and subjects the tissue to micro-deformation, which potently stimulates angiogenesis and fibroblastic migration. Other advanced adjunctive therapies, including hyperbaric oxygen therapy (HBOT) to reverse tissue hypoxia and electrical stimulation to accelerate cellular proliferation, are also utilised in refractory cases.
Surgical reconstruction: In severe cases involving extensive necrosis, exposed bone, or confirmed osteomyelitis, surgical intervention becomes mandatory. This process requires radical excisional debridement of all non-viable and infected tissue, frequently including an ostectomy of the underlying bony prominence (e.g., an ischiectomy to remove the mechanical focal point), followed by defect closure using highly vascularized myocutaneous flaps (e.g., gluteus maximus, gracilis, or VY hamstring advancement flaps). However, surgical intervention in elderly or medically fragile MS patients carries substantial morbidity and mortality risks, including severe blood loss and flap failure.
Spasticity management
The definitive treatment and surgical closure of pressure ulcers in patients with MS is virtually impossible without the rigorous control of spasticity. Spasticity and pressure ulcers often exist in a self-perpetuating positive feedback loop. A developing pressure ulcer acts as an intense, continuous nociceptive stimulus. Because the descending inhibitory pathways from the brain are damaged in MS, this peripheral noxious stimulus triggers severe, exaggerated spinal reflex arcs, exacerbating hypertonia and precipitating violent muscle spasms. These uncontrolled spasms, in turn, generate massive friction and shear forces against the support surface, physically tearing newly formed healing granulation tissue and driving the ulcer deeper into the muscle bed.
Surgical reconstruction of a pressure ulcer is destined for failure if post-operative spasticity is not aggressively managed. Muscle spasms make proper positioning of the limb to relieve tension on the suture line impossible. Uncontrolled hypertonia will rapidly cause mechanical tension across the surgical site, resulting in complete wound dehiscence, flap necrosis, and severe haemorrhage. Therefore, managing spasticity is not merely an adjunctive comfort measure; it is an absolute prerequisite to wound healing and surgical intervention.
The management of MS-related spasticity follows a stepped-care approach:
Physical and non-pharmacological interventions: Daily stretching routines, hydrotherapy, cryotherapy (cooling), and the use of specialised orthotics are the first lines of defence to maintain viscoelastic properties of connective tissue and prevent permanent joint contractures.
Oral antispasmodics: Pharmacological therapy typically begins with muscle relaxants. Baclofen (a GABA-B receptor agonist) and tizanidine (a central alpha-2 adrenergic agonist) are the mainstays of treatment. Clonazepam, diazepam, dantrolene, and gabapentin are also used, though their systemic side effects—particularly severe sedation, cognitive blunting, and hepatotoxicity— limit their utility in fragile patients.
Focal chemodenervation: For localised, severe spasticity affecting specific muscle groups—such as severe hip adductor spasms that prevent perineal hygiene and drive shear forces on the medial femoral condyles—targeted injections of botulinum toxin type A (e.g., Botox, Dysport) can be used.
Intrathecal therapy: In severe, generalised spasticity that is completely refractory to maximum tolerated doses of oral medications, the surgical implantation of an intrathecal baclofen (ITB) pump can be life-changing. By delivering micro-doses of baclofen directly into the cerebrospinal fluid of the intrathecal space, the therapy bypasses the blood-brain barrier.
Surgical and chemical denervation (rhizotomy and intrathecal phenol) and tenotomy.
Chemodenervation with Botox has largely replaced the need for rhizotomy or tenotomy for managing focal spasticity. Rhizotomy, or selective dorsal rhizotomy, manages focal spasticity by surgically disrupting the abnormal nerve signals that cause spasticity. During a selective dorsal rhizotomy, the surgeon leaves the so-called ventral (motor) roots intact so the patient does not lose the ability to move the muscle. Instead, they cut the dorsal (sensory) roots. The surgeon selectively cuts (sections) only the abnormal rootlets—often severing between 30% to 60% of them in the targeted area. The healthy rootlets are left alone. By reducing the amount of sensory input travelling from the muscle to the spinal cord, the reflex arc is dampened. The spinal cord stops sending excessive contraction commands to the muscle, effectively reducing the focal spasticity while preserving motor function and sensation.
Because selective dorsal rhizotomy permanently removes the faulty sensory pathways, it is one of the few treatments that can offer a permanent reduction in spasticity. It often leads to improved range of motion, easier positioning, better gait (walking), and reduced painful muscle spasms.
Another strategy is chemical rhizotomy using phenol. Intrathecal phenol can manage focal spasticity through chemical neurolysis (also called a chemical rhizotomy). Instead of surgically cutting the nerves, this procedure uses a strong chemical agent to intentionally damage and disable the specific spinal nerves causing the severe muscle tightness. Phenol is a chemical neurotoxin. When injected into the intrathecal space (the fluid-filled sac surrounding the spinal cord), it acts rapidly to denature (break down) the proteins in the nerve fibres. It strips away myelin and damages nerve axons. By chemically destroying the nerve roots that communicate with the spastic muscles, phenol completely blocks the hyperactive signals from firing, thereby relaxing the muscle.
You might wonder how an injection into the spinal fluid targets a focal (specific) area rather than paralysing the entire body. The secret lies in gravity and physics. Phenol is typically mixed with glycerin. This makes the solution “hyperbaric,” meaning it is heavier and denser than the surrounding cerebrospinal fluid (CSF). Because the solution is heavy, it sinks. During the procedure, the doctor places the patient on an X-ray or fluoroscopy table and tilts the patient’s body to very specific angles. Gravity causes the heavy phenol to flow downward and pool exactly over the targeted nerve roots (usually those controlling the legs or pelvis). The doctor leaves the patient in this tilted position for about 30 to 45 minutes to allow the phenol to “fix” to those specific nerves without spreading to healthy ones.
It is important to note that intrathecal phenol is a highly destructive and non-selective procedure. While selective dorsal rhizotomy carefully cuts only the sensory nerves to preserve the patient’s ability to move the muscle, phenol generally destroys both sensory and motor nerves in the area it touches. As a result, intrathecal phenol causes muscle weakness or paralysis and loss of sensation in the targeted area. Because it causes paralysis in the targeted muscles, intrathecal phenol is almost exclusively reserved for non-ambulatory patients (those who cannot walk) who have lost bowel and bladder function. In these cases, preserving motor function is no longer the primary goal. Instead, the phenol injection is used to relieve pain from chronic muscle spasms, prevent severe joint contractures, and improve the patient’s quality of life by making nursing care, hygiene, dressing, and wheelchair positioning significantly easier and more comfortable. The effects of phenol are often long-lasting (several months to years), though spasticity can sometimes return as the damaged nerves slowly regenerate.
Finally, tenotomy (tendon release) is an effective tool for managing the severe physical consequences of focal spasticity. Unlike a rhizotomy or phenol injection, which try to turn off the misfiring nerve signals, a tenotomy completely ignores the nervous system. It accepts that the muscle will continue to spasm and instead removes its ability to pull on the bones. During the procedure, a surgeon makes an incision and completely severs the tendon that attaches the spastic, contracted muscle to the bone. Because the tendon is under immense tension from the spastic muscle, severing it causes the two ends of the cut tendon to immediately snap apart, instantly releasing the tension on the joint. The muscle may still receive hyperactive signals from the damaged nervous system, leading it to continue contracting and spasm. However, because its mechanical anchor to the bone has been severed, that muscle no longer moves the joint or causes painful stretching. While tendon lengthening tries to preserve the patient’s ability to use the muscle, a complete tenotomy sacrifices the function of that specific muscle-tendon unit. Therefore, it is typically chosen when restoring normal movement is not the primary goal.
Tenotomy is recommended for severe, fixed contractures when a joint has been locked in place for so long that tendon lengthening is no longer physically possible. It is also done to prevent joint dislocation: Severe spasticity in the inner thigh muscles (adductors) can slowly pull the hip bone completely out of its socket. An adductor tenotomy releases this pull, keeping the hip joint safely in place. For non-ambulatory patients, severe spasticity can cause constant pain and make dressing, bathing, and sitting in a wheelchair incredibly difficult. Releasing the tendons allows the limbs to lie flat and relaxed, drastically improving daily comfort and care.
By sacrificing the mechanical connection of a problematic muscle, a tenotomy can prevent permanent joint damage and provide immediate relief to a localised area.
Pain management
Pain management in MS is often complex due to the presence of overlapping pain aetiologies. PwMS suffering from pressure ulcers routinely experience interacting neuropathic and nociceptive pain mechanisms, requiring targeted, multidimensional pharmacological strategies. Central neuropathic pain arises directly from damage to the brain and spinal cord; this pain is independent of external tissue damage. It is classically described as burning, shooting, tingling, or electric-shock-like. Because the neural pathways themselves are physically damaged or malfunctioning, this pain tends to be chronic, frequently worsens at night, and responds poorly to traditional nociceptive analgesics like NSAIDs or paracetamol. In comparison, nociceptive pain tends to be acute, arising directly from non-neuronal tissue destruction, such as the ischemic necrosis of the pressure ulcer itself, or the severe musculoskeletal strain and joint subluxation caused by unrelenting spasticity. It is mediated by intact, functioning peripheral nociceptors communicating the presence of tissue damage to the CNS.
Finally, nociplastic pain or hyperpathia is characterised by altered, amplified pain processing and central sensitisation in the absence of demonstrable new tissue damage. This diffuse, chronic pain amplifies the perception of both neuropathic and nociceptive stimuli, making routine preventative interventions—such as physical therapy, exercise, or simple repositioning by nursing staff—excruciatingly painful and difficult to tolerate.
Because a pressure ulcer serves as a continuous nociceptive driver that can amplify both central neuropathic pain and spasticity, silencing these pain signals is crucial for psychological well-being. However, conventional opioid narcotics are highly controversial, and their use is generally minimised. While opioids offer short-term nociceptive relief, they carry high risks of severe sedation, respiratory depression, and constipation. Opioid-induced constipation exacerbates neurogenic bowel dysfunction, increasing the risk of faecal impaction, overflow incontinence, and the subsequent bacterial contamination of the pressure ulcer. Instead, clinical management relies heavily on adjuvant analgesics that directly modulate nerve transmission. These include gabapentin, pregabalin and carbamazepine or oxcarbazepine, which are preferred for sharp, paroxysmal neuralgic-type pain.
Antidepressants, in particular tricyclic antidepressants (TCAs) like amitriptyline, or serotonin-norepinephrine reuptake inhibitors (SNRIs) like duloxetine, can be effective. They enhance the descending inhibitory pain pathways by increasing synaptic concentrations of serotonin and noradrenaline, providing dual relief for chronic neuropathic pain and can help with comorbid depression that frequently accompanies chronic pressure sores.
Occasionally, cannabinoid receptor agonists (THC and nabilone) can be tried not only for their analgesic properties against treatment-resistant neuropathic pain but also for their adjunctive anti-spasticity effects, offering a dual-mechanism approach to the pain-spasm cycle.
Non-pharmacological treatments, including transcutaneous electrical nerve stimulation (TENS), targeted physiotherapy, massage, and psychological interventions (such as cognitive-behavioural therapy), are used concurrently to help counteract psychological distress, fear, and anxiety associated with chronic pain and tissue loss.
UK regulation
Under the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014, service providers and registered managers are legally bound to notify the Care Quality Commission of specific adverse events that threaten patient safety. Regulation 18 explicitly targets the development of severe pressure ulcers. Under this regulation, providers must formally report the development of any pressure sore of Grade 3 or above that develops after the patient has been admitted to the facility or has started utilising the provider’s service.
The regulatory rationale classifies a Grade 3 or Grade 4 ulcer as a “serious injury.” To meet the threshold of a legally notifiable injury under this specific regulation, a healthcare professional must reasonably opine that the ulcer has resulted in:
Changes to the fundamental structure of the service user’s body.
An impairment of sensory, motor, or intellectual functions that is not likely to be temporary (defined explicitly as lasting, or likely to last, for a continuous period of more than 28 days).
The service user is experiencing prolonged pain or prolonged psychological harm (again, defined as lasting for at least 28 days).
A direct shortening of the life expectancy of the service user.
Crucially, the Care Quality Commission views compliance with these notifications as foundational to good governance. The CQC holds the statutory authority to move directly to criminal prosecution for breaches of these regulations if a provider fails to notify the commission “without delay,” or if the provider fails to demonstrate safe care and treatment (Regulation 12) resulting in avoidable harm.
In parallel with statutory CQC notifications, NHS England requires the meticulous, continuous logging of patient safety events through the National Reporting and Learning System (NRLS) and its successor, the Learn from Patient Safety Events (LFPSE) service. This framework mandates that pressure ulcers must be recorded regardless of their origin of acquisition. If a pwMS is admitted to an acute hospital with a pressure ulcer acquired in a community nursing home setting, the admitting hospital must still log the incident, clearly noting that it was present on admission, and transfer “ownership” of the record to the previous provider. This ensures unbroken epidemiological tracking across the entire health system and prevents critical incidents from falling through the gaps between community and acute care transfers.
The classification of harm within these systems has evolved significantly. Categories of pressure ulcers are no longer rigidly linked to preset degrees of harm (i.e., automatically categorising all Category 3 ulcers as “severe harm”). Instead, the actual clinical harm experienced by the patient dictates the classification, which ranges from no harm to death.
Historically, the UK utilised the Serious Incident (SI) Framework, under which organisations often automatically reported and investigated all Category 3 and Category 4 pressure ulcers via exhaustive root cause analysis (RCA). However, this automatic, reactive escalation proved administratively burdensome and counterproductive to patient care. The immense burden of conducting deep, time-consuming investigations into every severe ulcer—especially in patients with advanced MS where skin failure may physiologically occur despite perfect, flawless preventative care—diverted specialised tissue viability nurses away from active clinical management and into bureaucratic investigation roles.
In response, NHS England introduced the Patient Safety Incident Response Framework (PSIRF) in 2022. PSIRF represents a massive cultural and operational paradigm shift from mandatory, exhaustive investigations based on arbitrary harm thresholds to a highly proportionate, systems-based approach. Under PSIRF, organisations are no longer required to conduct extensive RCAs for all Category 3 and 4 ulcers if routine preventive measures and risk assessments are clearly documented. Instead, resources are strategically focused on analysing systemic clusters of incidents, explicit failures in the clinical pathway, or novel equipment failures, thereby accelerating actual systemic learning without overwhelming the frontline clinical workforce.
While clinical reporting mechanisms like LFPSE and PSIRF focus on systemic improvement and learning, the UK legal framework recognises a darker reality: the presence of a severe pressure ulcer can also be a physical manifestation of abuse, neglect, or profound institutional failure. Under the Care Act 2014, safeguarding adults is a statutory duty designed to help and protect individuals with care and support needs who are experiencing, or are at risk of, abuse and neglect, and are unable to protect themselves due to those specific needs.
In the context of tissue viability, neglect is defined as the deliberate withholding or the unintentional failure of a caregiver (whether a paid professional or an unpaid family member) to provide appropriate and adequate care. This encompasses a wide range of omissions, including ignoring clear physical care needs, failing to execute a mandated turning schedule for an immobile patient, withholding necessary pressure-relieving equipment, or failing to seek medical escalation when a Grade 1 ulcer is first noted, allowing it to deteriorate into a necrotic Category 4 wound. However, the Care Act 2014 explicitly clarifies that concerns regarding the general quality of a clinical service are not automatically safeguarding concerns under Section 42 of the Act. Historically, treating all severe ulcers as immediate safeguarding alerts resulted in a massive, unmanageable influx of referrals—with retrospective analysis showing that only approximately 20% actually required a full safeguarding investigation—threatening to completely paralyse local authority safeguarding teams and damaging relationships with clinical providers.
To rationally navigate the complex interface between clinical complications and true abuse, the Department of Health and Social Care, in partnership with the National Wound Care Strategy Programme, implemented a standardised National Safeguarding Protocol for pressure ulcers. When a severe pressure ulcer is identified, and neglect is suspected, an independent, practising registered nurse with specific wound care expertise—who was not directly involved in the patient’s immediate care at the time the ulcer developed—must complete the Adult Safeguarding Decision Guide within 48 hours of the ulcer’s identification.
This rigorous decision guide utilises a weighted scoring system based on six critical assessment domains 12:
Clinical deterioration: Tracking the speed of tissue breakdown, specifically if the skin deteriorated rapidly from healthy tissue to Category 3 or 4 since the last clinical visit.
Clinical condition: Evaluating whether recent systemic changes (e.g., severe MS relapse, acute systemic infection, end-of-life status) logically contributed to unavoidable tissue damage.
Care planning: Assessing whether a documented, appropriate risk assessment and prevention care plan was actively in place and adhered to.
Carer conduct: Identifying if an informal or formal caregiver willfully ignored needs, prevented access to health services, or refused to allow community nurses entry into the home.
Consistency: Determining if the severity and location of the tissue damage are disproportionate or inconsistent with the patient’s previously assessed risk status.
Consent and mental capacity: Investigating if a patient with full mental capacity actively refused life-saving interventions (such as turning or hoisting), or if care was delivered appropriately in the “best interests” of a patient lacking capacity under the Mental Capacity Act 2005.
A cumulative score of 15 or above on this guide, or severe overriding concerns raised through the independent nurse’s professional judgment, automatically triggers a formal safeguarding concern referral to the local authority’s adult safeguarding team. Accompanying this referral must be a detailed Body Map recording the exact anatomical site, dimensions (length, width, depth), and tissue typing of the ulcer, alongside photographic evidence obtained with appropriate sensitivity and legal consent.
Crucially, modern safeguarding protocols mandate a physiological distinction between systemic neglect and terminal, inevitable physiological decline. In advanced, end-stage MS, as the body begins to shut down, patients may experience Skin Changes at Life’s End (SCALE).14 SCALE recognises that during the active dying process, profound multi-organ hypoperfusion occurs. Blood is shunted away from the skin to preserve vital organs, making the skin and subcutaneous tissues inherently unstable and highly susceptible to ischemic death. In these specific physiological conditions, pressure ulcers become physiologically unavoidable despite optimal, flawless, intensive nursing care and the use of the highest specification support surfaces. If a post-incident review utilising the safeguarding framework determines that absolutely no omissions in care occurred and the rapid tissue damage is consistent with SCALE, the tissue damage is removed from punitive incident reporting systems. This vital distinction acknowledges that in the final stages of a devastating neurological disease, the clinical focus must shift entirely to palliative comfort, pain reduction, and dignity, rather than aggressive, medically futile preventative interventions that cause the patient distress.
Summary
When I started working in neurology over 30 years ago, I recall always having at least one or two patients on the neurology ward with pressure ulcers. Thankfully, this is now uncommon and typically occurs in the terminal phases of the disease. It has become rare because we now manage people with advanced MS much better than we used to in the past. This has been aided by technological innovations to prevent pressure sores (better chairs, mattresses, and beds) and by legislation protecting people with disabilities. The legislation has made nursing staff much more aware of the problem and the need for preventing pressure sores. I want to stress that patient education and self-monitoring have also played an important role.
I would be interested to know whether any of you have developed pressure ulcers and, if so, the context in which they occurred. How were they managed, and did they require surgical intervention?
If you think you are at risk of pressure sores and want more information, please contact your HCPs and get advice. Preventing pressure sores is far better than managing them.
Apologies for the length of the newsletter, but I need to balance the need to provide information with creating a comprehensive resource for pwMS. This newsletter will be transferred to the MS-Selfie microsite and will form a chapter in the MS-Selfie self-management guide.
Accidental readers
If you have been forwarded this email and are not an MS-Selfie subscriber, please consider subscribing and helping MS-Selfie expand its resources for the broader MS community. MS-Selfie relies on subscriptions to fund its curated MS-Selfie microsite, MS-Selfie books, MS-Selfie Infocards, and other activities that extend beyond the MS-Selfie Substack newsletters.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite and other related activities, as I don’t have time to do this myself. You must be a paying subscriber to ask questions unrelated to the newsletters or podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Questions
If you have questions unrelated to the newsletters or podcasts, please email them to ms-selfie@giovannoni.net. Prof. G will try to answer them as quickly as possible.
Important Links
🖋 Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have any problems, please tell your healthcare professional, who can help you.







