


Is it prime time for blood neurofilament level monitoring?
I am unsure if my killjoy colleagues have clocked just how significant the FDA’s Tofersen ALS decision is for the future of neurodegenerative disease diagnosis and treatment.

Several people have asked me what my highlights of the AAN 2023 meeting were. From an MS perspective, it has to be the observation that smoldering MS is now a mainstream concept. Smoldering MS has become firmly embedded in the MS lexicon and will therefore define future MS research (please see ‘Hot topic AAN 2023: smoldering MS’, 24-April-2023).

Outside of smoldering MS, there was the second positive RIS (radiologically isolated syndrome) trial (TERIS study), which showed teriflunomide delayed the onset of MS. 124 individuals were randomised, 89 who fulfilled the 2009 RIS diagnostic criteria to teriflunomide or placebo. Subjects on teriflunomide had a risk reduction in a CIS/MS-defining clinical event of 63% compared to placebo. During follow-up, 28 clinical events were detected, 20 in the placebo group and 8 in the teriflunomide group.
For me, the TERIS study results were expected and unsurprising (I gave the trial a 95-99% chance of being positive). Teriflunomide works in MS; why wouldn’t it work in RIS? I disagree with the current definition of MS based on a clinico- radiological worldview. MS is a biological disease defined pathologically. Therefore, people with RIS have MS, and teriflunomide, which has been shown to work in relapsing MS, will work in RIS.
The good news is that with two positive RIS trials showing dimethyl fumarate (DMF) and teriflunomide delay, the first clinical attack will change the definition of MS to include asymptomatic MS.
Another matter is whether regulators and payers will accept these changes to allow us to offer treatment to patients with RIS. Don’t forget time is the brain and spinal cord, so if you are diagnosed with RIS and have MS, why wouldn’t you want to have the option of going on to treatment? This is particularly relevant to the 10-15% of RIS patients destined to present many years down the line with PPMS. Starting on treatment when you have RIS will likely have an enormous impact on your levels of disability down the line.
At the AAN meeting, I was disappointed with the lack of discussion about EBV and its causal role in MS. Even in the MS update session at the end of the meeting focused on progressive MS, there was no mention of EBV. EBV is the hottest topic in MS and needs more air time.
Prof G’s AAN 2023 Highlight
The highlight of the meeting for me was the FDA’s decision to license Tofersen, an antisense oligonucleotide for a rare genetic form of motor neurone disease (MND) or amyotrophic lateral sclerosis (ALS). Tofersen reduces the synthesis of an enzyme called superoxide dismutase 1 (SOD1) protein in patients with mutations in SOD1. Everyone seemed surprised by FDA’s decision because the trial (see paper below) was negative on the primary outcome. However, Tofersen reduced plasma neurofilament light chain (NfL) levels at week 28 compared to the placebo arm. The FDA concluded that these findings are reasonably likely to predict a clinical benefit in patients with SOD1-ALS.
Many killjoys at the AAN criticised the FDA, saying yet again they overruled their advisory panel, which did not recommend Tofersen be licensed. I disagree with the killjoys for several reasons. Firstly, it looks like plasma NfL is a valid surrogate endpoint in ALS, i.e. it predicts outcome and is responsive to treatment. Secondly, there was a clear trend in relation to clinical benefit in the study, which became clearer in the extension study. And thirdly, the FDA only gave conditional approval under the accelerated approval pathway, which means more data will be required for Tofersen to keep its license. The FDA is also sending a message to the research and pharma community; we are prepared to meet you halfway and license DMTs in hard-to-test diseases with a huge unmet need. This not only incentivises the research community but gives people with neurodegenerative diseases hope.

The worst diagnosis a neurologist can make and give to a patient is MND or ALS. When I was a neurology registrar, my Professor and head of the Department told me I couldn’t become a neurologist until I had diagnosed, counselled, managed and buried my first patient with motor neurone disease. Kind of a baptism or brutal right of passage. It was brutal; I will never forget my first patient with MND. So having a licensed treatment, albeit for a very select number of patients with MND, is something that should be celebrated.
The Tofersen license is good news for MS because, by implication, the FDA has accepted plasma NfL as a validated biomarker, which means they are likely to accept it as a biomarker in other neurological conditions. This will almost certainly include raised NfL levels in presymptomatic SOD1-ALS patients. The latter could be extended to people at risk of MS. This is important for MS prevention trials. Suppose we accept raised blood NFL levels as part of the MS endophenotype. In that case, we can then use NFL levels as a biomarker to test whether interventions at a population level can prevent MS. NFL will give us an earlier readout, which is easier to measure in a large number of study participants than having to perform MRI scans and/or do clinical examinations.
The future
Now we have a validated biomarker of neuroaxonal damage, I envisage a future where people in the general population will have an annual Brain Health assessment. This will involve completing automated neurological, cognitive, visual, and auditory stress tests, completing a series of questionnaires, having a remote sleep assessment using a wearable device and having their blood NFL and other biomarkers measured. Those with abnormal results will undergo further investigations to see if they are in a specific neurodegenerative disease's presymptomatic or prodromal phase. If yes, they will receive disease-specific DMTs to slow the progression of their disease. All of this will happen before they have clinically manifest disease. It is no point waiting to become symptomatic to have a DMT; when you are symptomatic with Alzheimer’s or Parkinson’s, it is really too late to make much of a difference to the natural history of the disease.
I am unsure if my killjoy colleagues have clocked just how significant the FDA’s Tofersen ALS decision is for the future of neurodegenerative disease diagnosis and treatment. It hasn’t passed me by. Do you agree?
Paper 1
Background: The intrathecally administered antisense oligonucleotide tofersen reduces synthesis of the superoxide dismutase 1 (SOD1) protein and is being studied in patients with amyotrophic lateral sclerosis (ALS) associated with mutations in SOD1 (SOD1 ALS).
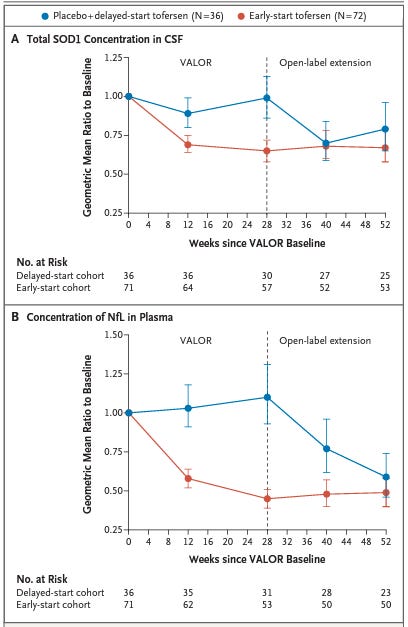
Methods: In this phase 3 trial, we randomly assigned adults with SOD1 ALS in a 2:1 ratio to receive eight doses of tofersen (100 mg) or placebo over a period of 24 weeks. The primary end point was the change from baseline to week 28 in the total score on the ALS Functional Rating Scale-Revised (ALSFRS-R; range, 0 to 48, with higher scores indicating better function) among participants predicted to have faster-progressing disease. Secondary end points included changes in the total concentration of SOD1 protein in cerebrospinal fluid (CSF), in the concentration of neurofilament light chains in plasma, in slow vital capacity, and in handheld dynamometry in 16 muscles. A combined analysis of the randomized component of the trial and its open-label extension at 52 weeks compared the results in participants who started tofersen at trial entry (early-start cohort) with those in participants who switched from placebo to the drug at week 28 (delayed-start cohort).
Results: A total of 72 participants received tofersen (39 predicted to have faster progression), and 36 received placebo (21 predicted to have faster progression). Tofersen led to greater reductions in concentrations of SOD1 in CSF and of neurofilament light chains in plasma than placebo. In the faster-progression subgroup (primary analysis), the change to week 28 in the ALSFRS-R score was -6.98 with tofersen and -8.14 with placebo (difference, 1.2 points; 95% confidence interval [CI], -3.2 to 5.5; P = 0.97). Results for secondary clinical end points did not differ significantly between the two groups. A total of 95 participants (88%) entered the open-label extension. At 52 weeks, the change in the ALSFRS-R score was -6.0 in the early-start cohort and -9.5 in the delayed-start cohort (difference, 3.5 points; 95% CI, 0.4 to 6.7); non-multiplicity-adjusted differences favoring early-start tofersen were seen for other end points. Lumbar puncture-related adverse events were common. Neurologic serious adverse events occurred in 7% of tofersen recipients.
Conclusions: In persons with SOD1 ALS, tofersen reduced concentrations of SOD1 in CSF and of neurofilament light chains in plasma over 28 weeks but did not improve clinical end points and was associated with adverse events. The potential effects of earlier as compared with delayed initiation of tofersen are being further evaluated in the extension phase. (Funded by Biogen; VALOR and OLE ClinicalTrials.gov numbers, NCT02623699 and NCT03070119; EudraCT numbers, 2015-004098-33 and 2016-003225-41.).
Subscriptions and donations
Paid subscriptions to MS-Selfie are being used to administer the Newsletter and associated MS-Selfie microsite, which is now open to all readers. At the request of several readers, I have now added the option of making a one-off donation. To keep this initiative open to all readers, I would appreciate it if those who can afford a subscription to subscribe. For active paying subscribers, thank you; your contribution is much appreciated. Because of the falloff in paying subscribers, I am considering returning to a paywall that will give paying subscribers six months of unlimited access to all newsletters. At the same time, free subscribers will have a wait to access the newsletters later, not as an email, but on the substack site.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your own healthcare professional, who will be able to help you.
Very thought-provoking, Gavin.
I'm 60 and perhaps 10 years into PPMS, having also had Mononucleosis (Glandular Fever) at 19. I have a daughter of 27 and son of 19 who are showing no signs of MS, thankfully. Statistically they have approx. 2-4% probability of contracting MS themselves.
The question is, should I get them screened for RIS and where should I go for that?
All this sounds like exciting news and a more positive outlook for those with neuro degenerative disorders. Almost certainly too late for me but hope for my grandchildren.