


HPV vaccination to prevent reinfection
Several patients who have been HPV positive have asked whether or not they should get vaccinated to protect themselves from other strains of the virus.

I always stress the importance of derisking disease-modifying therapies as best you can before starting treatment. For example, we try to insist that patients have an up-to-date cervical smear or vaginal human papillomavirus (HPV) PCR to exclude active HPV infection before starting alemtuzumab. In reality, we should be doing this with all chronic immunosuppressive therapies, particularly the S1P modulators (fingolimod, siponimod, ozanimod, ponesimod).
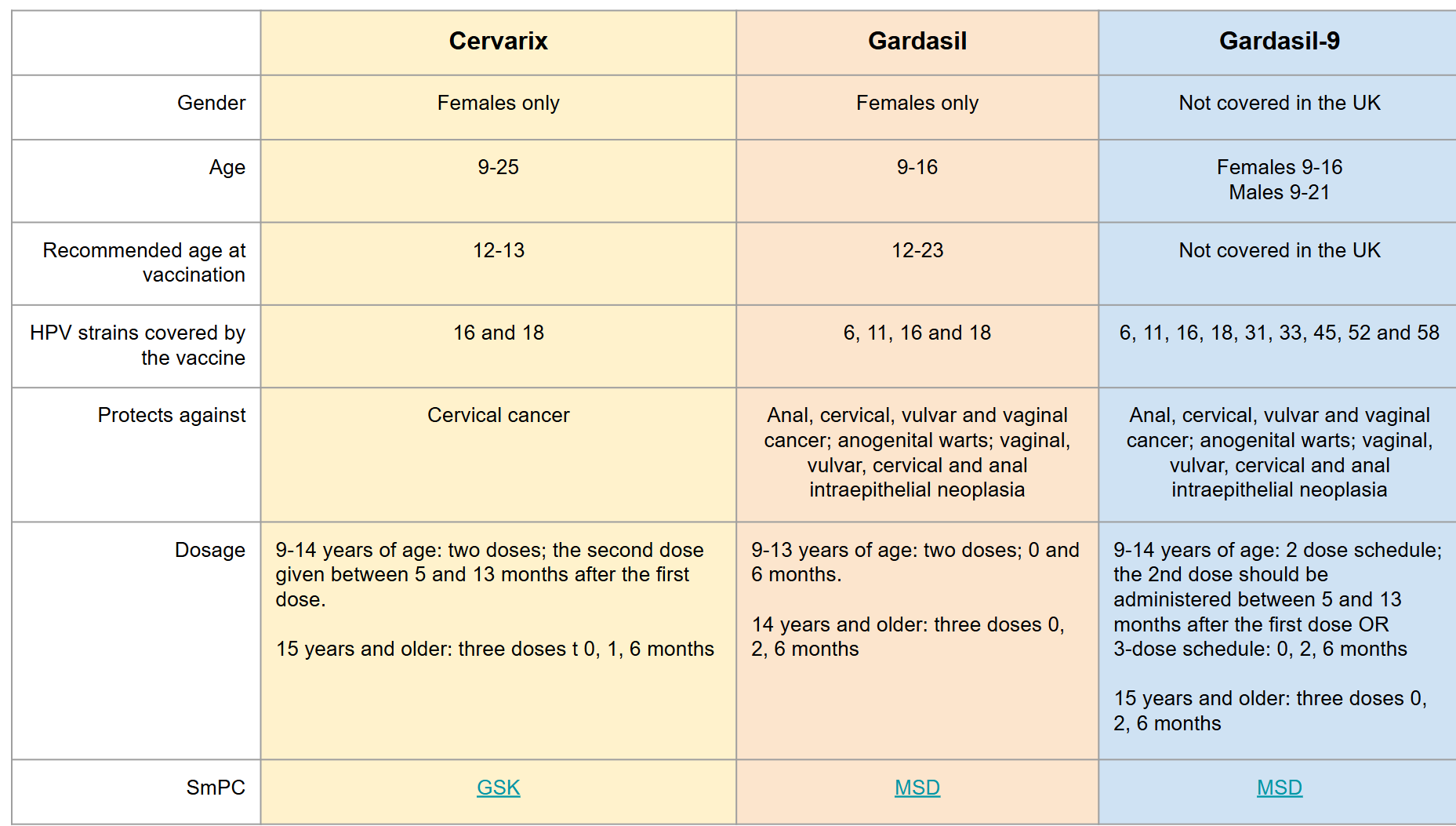
Another issue is having or upgrading your HPV vaccine status. Most people with MS who had the HPV vaccine would have had the quadrivalent vaccine that only covers four strains of HPV (Gardasil-4). The nonavalent Gardasil-9, covering nine oncogenic strains, replaced Gardasil-4 in the Summer of 2022. Please note that the national prevention programme started for girls in school year 8 in the summer of 2008. The NHS only expanded the HPV vaccination program to include all boys in school year 8 from September 2019. If you were in the above cohorts and missed your vaccine, you are eligible for it under the NHS. However, if you are not in the eligible cohorts and want to upgrade your vaccine status from Gardasil-4 to 9 or decide to have the vaccine for the first time, you must pay for it privately.
Please note that HPV also cause other cancers (oral, throat, oesophageal, penile, anal and rectal) and warts. Having good immunity to HPV before starting an immunosuppressive therapy makes sense. Do you agree?
Please see the prior MS-Selfie Newsletters for more information:
Case study: cervical intraepithelial neoplasia (CIN) and ocrelizumab (6-Nov-2021)
The rationale for derisking DMTs (20-Aug-2021)

Another issue is what if you detect the virus with a cervical smear and/or vaginal swab? In the past, we usually delayed starting treatment until the gynaecologists treated the problem and gave us the all clear to start treatment. The same advice should apply to perineal or cutaneous warts. There have been many case reports of patients with warts who, when started on alemtuzumab or fingolimod, develop disseminated warts that are difficult to treat. The same goes for other infections, for example, molluscum contagiosum, hepatitis B & C, TB, …
Several patients who have been HPV positive have asked whether or not they should get vaccinated to protect themselves from other strains of the virus. I have always said yes, and I have argued that the vaccine may work as an immunotherapy against the HPV strain they already have, helping to eliminate it or preventing it from recurring after cervical surgery. However, there has been little data to support this advice. However, the paper below that has recently been published shows that women undergoing surgical procedures for HPV-associated cervical lesions (either low-grade cervical intraepithelial neoplasia (CIN)-1 or high-grade CIN2-3) who received the 9-valent HPV vaccine after treatment had significantly lower rates of positive HPV tests compared to those who were not vaccinated. This indicates that administering the vaccine as an additional measure after surgery can help clear or reduce the persistence of HPV infections, potentially lowering the risk of lesion recurrence.
Besides the already established benefits of primary prevention (vaccination before exposure) and secondary prevention (screening), the study supports the idea that immunisation may serve as an effective tertiary prevention tool. This means it can help prevent new HPV infections or reactivation after treatment for pre-existing lesions. Implementing post-treatment vaccination could decrease the number of follow-up visits, colposcopic examinations, and subsequent treatments. This would benefit patient health and reduce the burden on healthcare systems.
The study stratifies patients by age (< 40 and ≥ 40 years) and finds statistically significant benefits, particularly in women aged 40 and above with low-grade lesions. Even though the effect in high-grade lesions was not significantly different in the age-based analysis, overall trends support the positive impact of vaccination post-treatment. This result emphasises that the vaccine can be beneficial irrespective of age, suggesting that health policies should not automatically restrict vaccination to younger groups only, but include older women recovering from cervical procedures.
The study adds evidence that could influence future clinical guidelines by recommending the inclusion of post-treatment HPV vaccination as a standard care practice. Utilising the vaccine after surgery might help maintain lower HPV positivity rates and eventually reduce the risk of cervical cancer development, taking a more comprehensive approach to patient care. By incorporating these findings into clinical protocols, HCPs can offer patients more robust protection against recurrence and subsequent HPV-related complications.
When vaccination significantly reduces recurrent lesions, the overall cost of long-term care may be reduced. This implies fewer invasive procedures, less need for repeat examinations, and consequent cost savings for healthcare providers and governments. The question is whether or not the NHS will be convinced, or if a larger randomised study will be needed to confirm these findings. I suspect the latter. However, if I were a woman with active HPV infection with premalignant cervical lesions, I would want the vaccine and would probably find the funds to pay for it privately. Who said healthcare is equitable?
Please let me know if you have elected to have the HPV vaccine and/or upgraded your vaccine status with the new Gardasil-9 vaccine. I know this issue is complicated, but it is all about prevention rather than dealing with a potentially serious problem later.
Introduction: The effectiveness of post-treatment HPV vaccination with the Human papillomavirus 9-valent (9vHPV) vaccine in women treated with loop electrosurgical excision procedure (LEEP) for high-grade cervical intraepithelial neoplasia (CIN2-3) or laser ablation (LA) for low-grade lesions (CIN1) remains a topic of ongoing research.
Study design: This single-center retrospective observational study included 326 women aged 25 to 65 years who underwent surgical treatment between 2020 and 2024. Participants were divided into two groups: vaccinated (V) and non-vaccinated (NV). A further stratification was then reported by age < 40 years (n = 174) and ≥ 40 years (n = 152). The primary outcomes were HPV test results and colposcopy findings 6-15 months post-treatment, evaluating the potential adjuvant effect of HPV vaccination.
Results: The vaccinated group (V-group) comprised 68 % (222/326) of participants, while 32 % (104/326) were unvaccinated (NV-group). Among women treated for CIN1, a positive HPV test was detected in 38 % of unvaccinated women compared to 18 % in vaccinated women (p = 0.0169). Among those treated for CIN2-3, 18 % of unvaccinated women had a positive HPV test, compared to 8 % in the vaccinated group (p = 0.0353). Vaccination, also in women with an age ≥ 40-year-old had a statistically significant effect in reducing the proportion of women with a positive HPV test (p = 0.0100).
Conclusion: Human papillomavirus 9-valent vaccine was associated with a significant reduction in the proportion of women with a positive HPV test. These findings support its potential role in tertiary prevention of HPV-related cervical disease, particularly in reducing HPV persistence after surgical treatment.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. You must be a paying subscriber if people want to ask questions unrelated to the Newsletters or Podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
🖋 Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.
I'm 62, had MS for 20 years. Since being on fingolimod (6 years), I've tested positive for HPV. I've been seeing my gynaecology dept at my local hospital for the same time. I test positive for HPV after every annual smear test, despite there being no evidence of abnormal cells. I have raised the issue of being on fingolimod and there being evidence that it may heighten my chances of being HPV positive (I have presented the gynaecology dept with several papers covering the issue). I took matters into my own hands and managed to get the latest HPV vaccination done last year (my neurologist on my clinical trial (Sizomus) organised it for me, and I was questioned every step of the way by medical professionals who queried why I wanted the HPV vaccine). Didn't work. I've just undergone my third colposcopy procedure because I am still testing positive for HPV, under general anaesthetic (not pleasant). That doesn't seem to be solving the HPV problem either. Not sure what else I can do.
I looked into vaccination after clearing an HPV infection. It's too expensive sadly 😥