


How to avoid a DMT cul-de-sac?
You should try to push back from being labelled as having SPMS or PPMS to prevent limiting your treatment options.

As we move towards a biological definition of multiple sclerosis (MS) and away from the three-, four- or five-disease classification system that has been in place since the late 80s, dare I suggest you take control of your own MS classification?
Classifying MS as being asymptomatic MS or radiologically-isolated syndrome (RIS), prodromal MS, clinically isolated syndrome (CIS), relapsing-remitting MS, transitional MS, relapsing secondary progressive (rSPMS), non-relapsing SPMS (nrSPMS) or primary progressive MS (PPMS) needs to become history. These labels have significant implications for which disease-modifying therapies you can or cannot receive. For example, on the NHS, once you get labelled as SPMS, you can only potentially receive siponimod. Similarly, once you get labelled as having PPMS, you can only potentially receive ocrelizumab. This is why these are dead-end DMTs or cul-de-sac DMTs.

We now know that the biology of MS is the same across the disease spectrum and what determines your clinical phenotype is superimposed focal inflammation (relapse and focal MRI activity), smouldering MS (worsening not attributable to focal inflammation), and your reserve capacity, i.e. the ability to recover function or compensate for existing damage.
MS is one disease, and what matters diagnostically is whether or not you have MS. Once you have a diagnosis of MS, you need to know if your disease is active, i.e. recent relapses or focal MRI activity, which makes you eligible for anti-inflammatory therapies. In addition, you need to see if you have smouldering MS, i.e. worsening that is not due to overt focal inflammation. Treatment of smouldering MS requires a different therapeutic strategy with CNS-penetrant therapies targeting CNS mechanisms of smouldering disease.
You should try to push back from being labelled as having SPMS or PPMS to prevent limiting your treatment options. Try to get your HCP to label you as having MS and keep the descriptors simple and without using the adjective progressive. This will become increasingly relevant over time as we develop combination therapies to target both components of our treatment target.
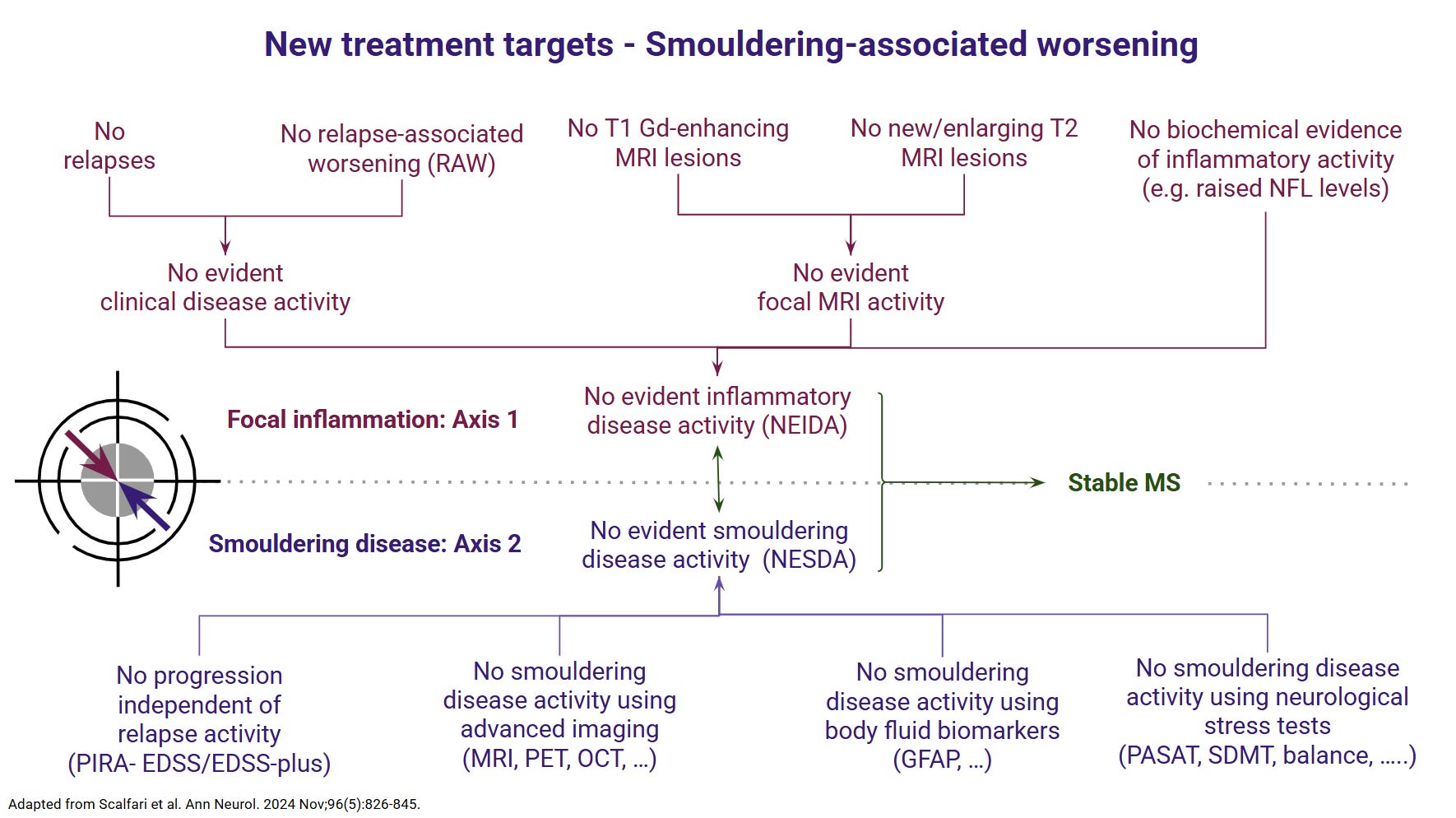
The following figures illustrate the new emerging classification system of MS and treatment targets.

I would be interested to know if any of you have attempted to get your MS relabelled MS instead of being pigeonholeed in having SPMS or PPMS. Would this be a discussion your HCPs would entertain? How do you feel about dropping the term progressive as a descriptor?
Progression in the context of MS is a misnomer. Progression means improvement or advancement. However, when it is applied to MS, it either means worsening disability or labelling someone as having another type of MS. Both these uses of the word are incorrect.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are available free of charge. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. You must be a paying subscriber to ask questions unrelated to the Newsletters or Podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
🖋 Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you experience any problems, please consult your healthcare professional, who will be able to assist you.
Thank you. My doctor didn't want to write that I am SPMS (although clearly I am progressing with no relapses or MRI changes), and he said "Once we write SPMS, the ship has sailed, there is no coming back, and you will be limited to siponimod only".
I am glad that he thought that way, because I received Mavenclad ;-)
I believe personally, that if we have MS, then that's what it should be called. There's no need to label it as RRMS or SPMS, because there's no need to differentiate. Similarly there's no need to say you have 'active disease' because we should all be treated the same. One of the main reasons, is that those of us who have been told that we show no signs of active lesions at the time of their MRI, are made to feel that they are not as as bad as those who have active lesions, and therefore are denied a treatment. I think that however far we've come on our individual journey's, it should be called MS. I believe that too much of the research being done, is focused on the basis of 'what stage' we are at, whereas it should be focused on 'how far into our individual journey's we are, and how it affects our daily life. Then, if we're happy to try a treatment, we should be allowed to.