
Can we cure MS?
The only way to find out is to define an MS cure and to look for it.

I am currently working on a paper with a few colleagues to build consensus on what an MS cure looks like. We last defined a cure in 2013, and things have moved on since then. We need to define a cure to determine whether any of our treatments lead to a cure; without a working definition, we are looking in the dark.
To be cured of having MS, you need to have MS as defined by our diagnostic criteria, be off treatment for a period of time and have no evidence of inflammatory disease activity (NEIDA), no evidence of smouldering associated worsening or ongoing end-organ damage, no chronic active lesions (slowly expanding lesions or paramagnetic rim lesions) and we are also proposing you need to lose the intrathecal or spinal fluid oligoclonal IgG bands that we think are pathogenic in MS. The problem with chronic active lesions and OCBs is that they can take years or even decades to disappear. This is why an MS cure can only really be defined in the future.
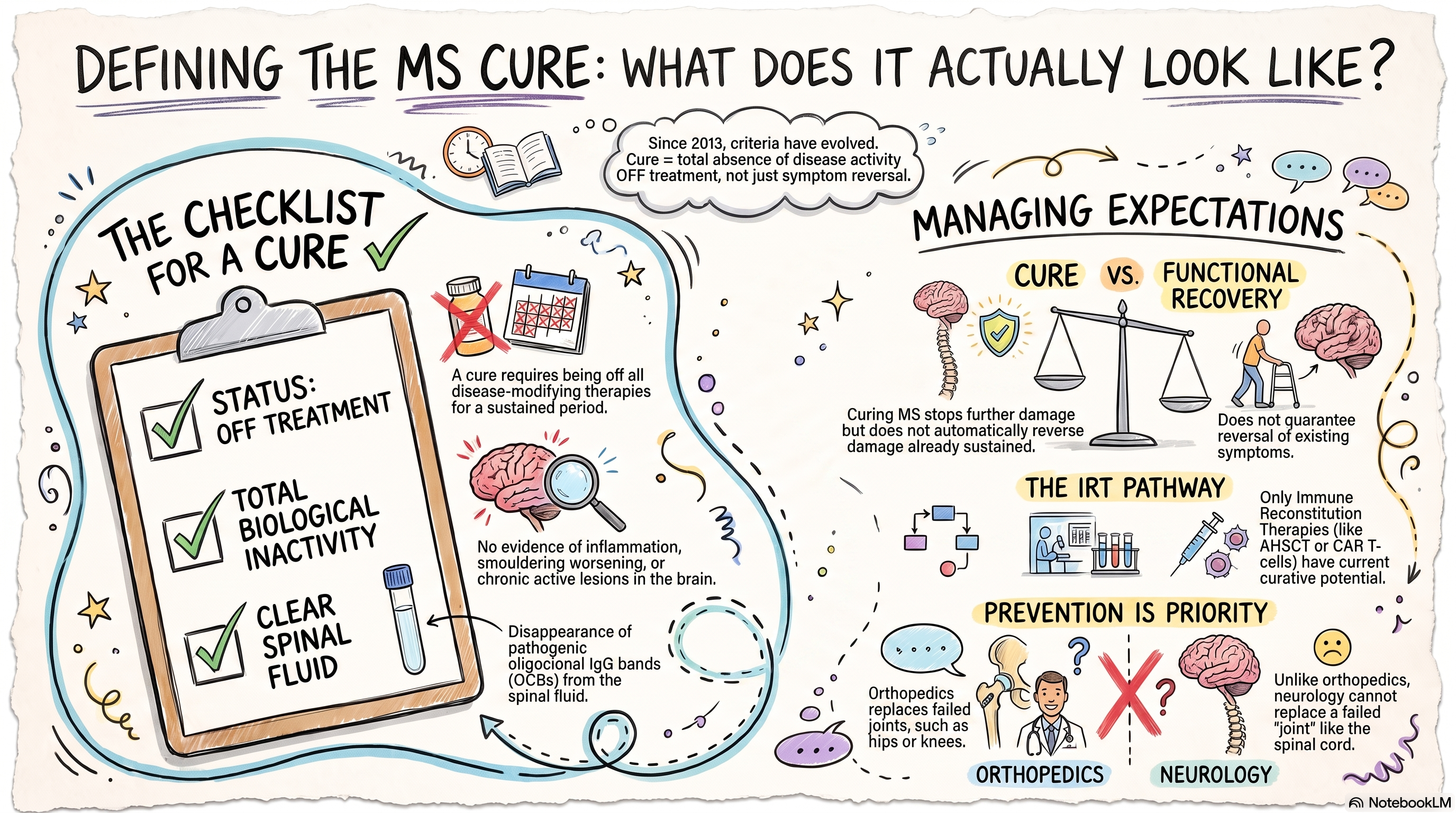
Being off treatment is a difficult one to get your head around. How can you be cured of a disease if you are still on a treatment for that disease? In reality, the only treatments that can cure MS are the immune reconstitution therapies, i.e., alemtuzumab, cladribine, AHSCT, and, more recently, CD19-targeted CAR T-cells. I only add CD19-targeted T-cells to the list because they have the potential to purge the body of EBV, which is likely the cause and driver of MS.
An important practical corollary is that a cure for MS is not the same as functional recovery. Curing one of MS prevents further damage but does not, of itself, necessarily reverse damage already sustained. Therefore, managing the expectations of people with MS, i.e. distinguishing ‘no more disease’ from ‘restoration of lost function’, is central to the responsible use of the term MS cure.
I still receive emails from people with MS who are being denied the option of having an IRT because their HCPs are not comfortable prescribing alemtuzumab, cladribine or AHSCT. I have referred to these people as refuseniks. However, if we can show that a proportion of pwMS treated with an IRT are cured of having MS, then maybe the refuseniks will disappear. Please read my old newsletter on the refuseniks to see if anything has changed Refuseniks-2 (Mar 04, 2022).
I have always pushed for the early effective treatment of MS and more recently for flipping the pyramid. The purpose of disease modification is to prevent end-organ damage. Sadly, we don’t have therapies licensed to reverse end-organ damage, which is why prevention makes sense. Similarly, if we can cure someone of having MS, why would we not try? I suspect many of you will disagree.
Just to say I have finally succumbed to my pain and increasing disability and had my failing right hip replaced last Friday. Orthopaedic surgeons have the option of replacing a failed joint; in neurology, we can’t give you a new spinal cord or restore lost brain stem functions or reverse your cognitive deficits. All we can do is prevent them from being damaged in the first place and try to maximise their function so you can reach old age with as much reserve as possible. Our aim to try and allow you to age as normally as possible.
Accidental readers
If you have been forwarded this email and are not an MS-Selfie subscriber, please consider subscribing and helping MS-Selfie expand its resources for the broader MS community. MS-Selfie relies on subscriptions to fund its curated MS-Selfie microsite, MS-Selfie books, MS-Selfie Infocards, and other activities that extend beyond the MS-Selfie Substack newsletters.
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS-Selfie microsite and other related activities, as I don’t have time to do this myself. You must be a paying subscriber to ask questions unrelated to the newsletters or podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Questions
If you have questions unrelated to the newsletters or podcasts, please email them to ms-selfie@giovannoni.net. Prof. G will try to answer them as quickly as possible.
Important Links
🖋 Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have any problems, please tell your healthcare professional, who can help you.
As an MSer, I’d just like to say that I appreciate you and all your effort. Thank you.
Thanks as ever for the post. Congrats on new hip and all the best for a great recover!. J 🙂