


Breaking news: we have a new therapeutic target in MS
The phase 2 results of the Frexalimab (anti-CD40L) study are strikingly positive. What does this mean for MS?

Did you read MS-Selfie Research Newsletter on ‘Closing in on the Cause of MS by Dissecting the Immunology of MS Disease-Modifying Therapies’ (25-May-2023)? If not, I would urge you to do so, as it gives the backstory to this newsletter.
I conclude the newsletter by discussing an immune pathway highlighted by our group and others involving CD40 and its binding partnering, the CD40 ligand (CD40L).
CD40 is a critical costimulatory signal that drives T-cell activation and is involved in B-cell and innate immune activation. As the CMSC has started and the embargo lifted, I can now tell you the phase 2 Frexalimab study results are strikingly positive. These results are the most exciting to emerge in MS in the last 12-24 months. It is also hard to believe that the AAN turned down our abstract as a late-breaker (what is happening to the AAN?).
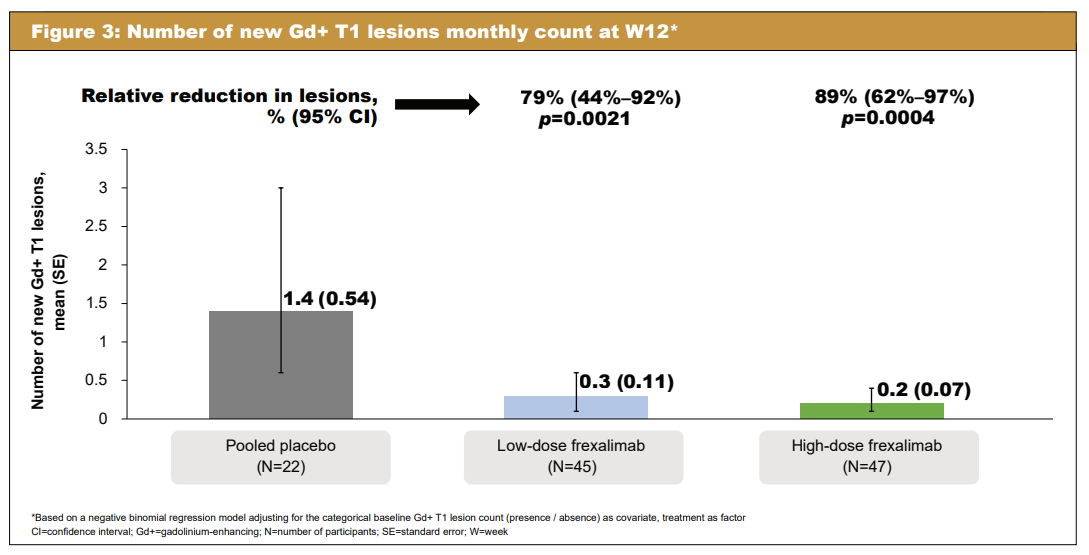


You are welcome to download a press release from Sanofi or the poster.
These results say a lot about the pathogenesis of MS? Do these results confirm a critical role for T-cells in the pathogenesis of MS and prove MS is an autoimmune disease unrelated to ongoing EBV infection? Because I am convinced that EBV causes MS and that continued EBV latent-lytic cycling drives MS disease activity, these results need to be interpreted in the context of EBV.
It is no surprise to evolutionary virologists that EBV has hijacked CD40 and the CD40-ligand signalling pathways. Latent membrane protein 1 (LMP1) mimics CD40 to augment the normal CD40 signalling pathway. This gives EBV-infected cells a survival advantage. Blocking the normal CD40 pathway with Frexalimab may be enough to kill EBV-infected B-cells or at least inhibit their functioning.

It has also been noted that EBV-infected B-cells express CD40L (Imadome et al. Proc Natl Acad Sci U S A. 2003 Jun 24;100(13):7836-40). Non-infected B-cells don’t express CD40L. This aberrant CD40L expression may augment EBV-infected B-cell's ability to present antigens, even autoantigens. Blocking CD40L on EBV-infected B-cells will interfere with B-cell antigen presentation by these EBV-infected cells. So, anti-CD40L may be working in MS via mechanisms linked to EBV. We must explore EBV biology in phase 3 Frexalimab clinical trials.

Even if I am wrong about EBV and Frexalimab, there is no doubt the results of this study will send a buzz through the MS community, particularly the immunologists and genomics experts who predicted these results decades ago.
Could Frexalimab be doing more? Will Frexalimab put pwMS into long-term remission and mimic the stunning results we see with alemtuzumab or AHSCT? Blocking CD40-CD40L interactions should convert a T-cell activating signal into a tolerogenic signal and stop autoimmunity. This is why I am so excited about Frexalimab as a potential treatment for MS.
I am aware that the information in this newsletter is hardcore immunology, but I think you need to be mindful of the basics so you can share my enthusiasm. Please ask questions if you don’t understand anything.
Epstein-Barr virus (EBV), implicated in numerous human diseases, including lymphoid malignancies, persistently infects peripheral B cells and transforms them into lymphoblastoid cell lines. Here we found that EBV equally infected B cells from patients with X-linked hyper IgM syndrome and those from healthy donors; however, it hardly transformed X-linked hyper IgM syndrome B cells, because of the dysfunctional gene of CD40 ligand (CD40L) of the patients. Unlike CD40, CD40L is not usually expressed on B cells. However, we found that EBV infection of normal B cells induced CD40L expression as a critical effector in host cell transformation and survival. Moreover, chronic active EBV infection of peripheral T cells, implicated in T cell malignancies, was associated with ectopic expression of CD40, and, in Jurkat T cells, EBV infection induced CD40 expression. These results suggest that EBV infection induces CD40L/CD40 signaling in host cells, which appears to play an essential role in its persistent infection and malignancies of lymphocytes.
Subscriptions and donations
Paid subscriptions to MS-Selfie are being used to administer the Newsletter and associated MS-Selfie microsite, which is now open to all readers. At the request of several readers, I have now added the option of making a one-off donation. To keep this initiative open to all readers, I would appreciate it if those who can afford a subscription to subscribe. For active paying subscribers, thank you; your contribution is much appreciated. Because of the falloff in paying subscribers, I am considering returning to a paywall that will give paying subscribers six months of unlimited access to all newsletters. At the same time, free subscribers will have a wait to access the newsletters later, not as an email, but on the substack site.
General Disclaimer: Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Barts and The London School of Medicine and Dentistry nor Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your own healthcare professional, who will be able to help you.
I'm 56. I'll be dead before anything comes to market to help me lol. Good news for those coming up behind though and those who haven't yet been diagnosed.
Please can I have some Frexalimab. I have been reading about MS research since I was diagnosed age 30 when my son was 2. He is now 38 and I have just filled in the form to claim my state pension. Just give me the drugs.....PX