



Anyone who lives in London will tell you that buses come in threes. What you are not told is which bus to catch and which buses to miss.
I have just turned 60, and I have the option of choosing between three buses. I need to decide which one to catch.

I suspect it is quicker to catch the second bus as the first one is usually packed and stops frequently and longer to allow passengers to get on-and-off. This may enable the second bus to overtake it as it doesn’t have to stop at each bus stop. The third bus may be the emptiest, so it catches up quickly to the first two but is unlikely to overtake the second bus that is now in front.
The first bus is to continue doing what I do now, and I hope I survive trying to run an increasingly busy NHS MS practice, conduct clinical trials, maintain MS-Selfie, and set up a new line of research around EBV and MS prevention.
The second option is to step back from clinical practice and use the time to focus on MS prevention. The third and final option is to throw in the towel and retire early to focus on my family and interests outside of medicine.
Many of my colleagues are taking up the third option; burnt out and exhausted, they want something different.
I have been told things happen for a reason, so I have had to make a tough decision. My accident and its lingering effects on my day-to-day functioning, the threat of melanoma metastases, clinical burnout and increasing administrative demands have led to me to the decision to take partial retirement. So, starting on the 1st of September 2024, I will stop NHS clinical practice and work four days a week. The latter is a requirement of the NHS partial retirement scheme.
I will continue to do MS clinical trials and see potential study subjects. Clinical trials are vital as each trial is an experiment and, if designed and done well, allows you to formulate, reject or advance a research hypothesis. I am particularly interested in exploring EBV antivirals and immunotherapies as potential treatments for MS.
I recently gave an invited talk at the Medical Society of London entitled “Multiple Sclerosis—a road less travelled, with miles to go before I Sleep”. The lecture was part of the Mansell Competition for young researchers, which our brilliant Dr Ben Jacobs won. He summarised his PhD work on the genetic analysis of MS risk in diverse ancestral populations.
In my talk, I discussed what still needs to be done to prove that EBV is the cause of MS. I presented the obvious MS prevention trials that need to be undertaken. I am involved with most of the EBV MS prevention strategies to a greater or lesser extent, but the one most neglected is infectious mononucleosis (IM).
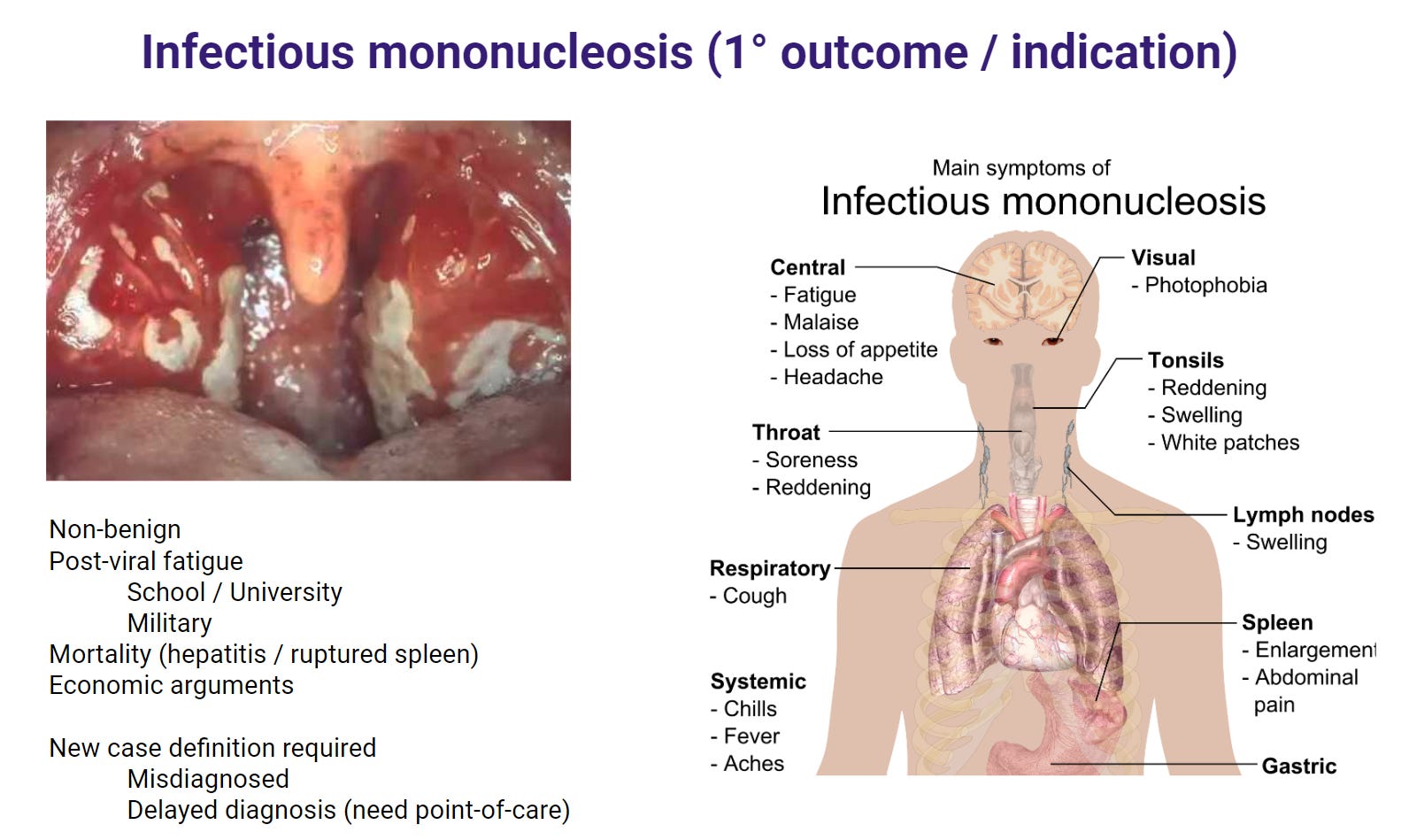
The hypothesis is simple. IM or symptomatic EBV infection is the predominant risk factor for the development of MS. People who have IM are about 2.0-2.5 times more likely to develop MS. Why? I suspect the aberrant immune response during IM is the substrate that sets the stage for autoimmunity in the future. If we can diagnose and treat IM with effective antiviral drugs and prevent this immune response, we can avoid the development of MS and other EBV-related autoimmune diseases. The analogy is streptococcal infections and post-streptococcal autoimmunity, for example, rheumatic fever. Rapidly diagnosing and treating streptococcal pharyngitis and impetigo have virtually eliminated rheumatic fever in high-income countries. Could treating infectious mononucleosis do the same for MS?
I have been awarded a grant from the Horne Family Foundation to set up a pilot study to see if we can create a rapid diagnosis and treatment pathway for purulent pharyngitis, which will include IM. This will allow us to study the immunology of IM and conduct randomised controlled trials in patients with acute IM. If we can get a licensed therapy for acute IM, we will then set up population-based registers to see if treating IM reduces the incidence of MS and other EBV-related disorders. This is not dissimilar to what we want to achieve with a prophylactic EBV vaccine.
My partial retirement is a misnomer. I will use the time freed from stopping clinical work to do something completely different: MS prevention.
How will this affect my patients? People with MS who are from out of the area and are not being treated at Barts Health will need to be followed up and managed by their local MS team. I have stopped taking new referrals. My colleagues at Barts Health have kindly agreed to take over some of my patients, and a close colleague of mine will be taking over my general neurology and MS clinic later this year. In the interim, I will continue to run and contribute to MS-Selfie, but I will be looking for someone to help me with a view of a timely succession. I still plan to complete the MS-Selfie microsite and launch the MS-Selfie self-management course and guide.
People are surprised that despite my commitment to neurology and multiple sclerosis, I do have outside interests. I intend to allocate more time to these pursuits. Having had two life-threatening events in short succession focuses the mind on one's mortality. I have many miles to go before I sleep and promises to keep …..
You can download my slides from my Medical Society of London talk here and watch a recorded version on my YouTube channel.
If you have any comments or questions about my London bus choice, please let me know.
Finally, I have recently been asked to start a series of online webinars and live Q&A sessions. For example, I could do the first one on the issues discussed in this newsletter. Is there an appetite for live sessions?
P.S. For patients under my care, please don't panic. We will process your cases individually and then set up a follow-up plan. Either a referral back to your local team, a transfer to one of my colleagues, or you will stay in my clinic, which will be taken over later this year by a close colleague. I am not physically leaving and will still see trial subjects at the Royal London Hospital and will be participating in the multidisciplinary team meetings (MDTs).
Subscriptions and donations
MS-Selfie newsletters and access to the MS-Selfie microsite are free. In comparison, weekly off-topic Q&A sessions are restricted to paying subscribers. Subscriptions are being used to run and maintain the MS Selfie microsite, as I don’t have time to do it myself. You must be a paying subscriber if people want to ask questions unrelated to the Newsletters or Podcasts. If you can’t afford to become a paying subscriber, please email a request for a complimentary subscription (ms-selfie@giovannoni.net).
Important Links
X (Twitter) / LinkedIn / Medium
General Disclaimer
Please note that the opinions expressed here are those of Professor Giovannoni and do not necessarily reflect the positions of Queen Mary University of London or Barts Health NHS Trust. The advice is intended as general and should not be interpreted as personal clinical advice. If you have problems, please tell your healthcare professional, who will be able to help you.









Prof G is retiring